
The Neurobiology of the “Fourth Trimester”
The study of neonatal sleep architecture what parents commonly call a “newborn sleep schedule” represents one of the most complex frontiers in developmental chronobiology.
As your infant transitions from the constant, buffered environment of the womb to the external world, their biological imperative shifts. They must move from passive synchronization with the mother to the independent entrainment of their own internal oscillators. For the researcher in neonatal physiology, this transition is not merely a behavioral milestone; it is a profound neurobiological maturation of the Suprachiasmatic Nucleus (SCN), the master circadian pacemaker located within the anterior hypothalamus, which acts as the biological foundation for any future newborn sleep schedule.
During the first twelve weeks of life, the human infant undergoes a systematic reorganization of sleep states. They move from a polyphasic, ultradian-dominant pattern (short, frequent cycles) to a consolidated circadian rhythm.
This report serves as an exhaustive scientific resource. We will synthesize clinical data from the American Academy of Pediatrics (AAP) and the National Institutes of Health (NIH) to elucidate the mechanisms of sleep, the chemistry of gastrointestinal soothing, and the stringent safety protocols required to mitigate the risk of SIDS in 2026.
Table of Contents
The Neurobiology of Neonatal Sleep Cycles
The human newborn enters the world with a sleep architecture that is fundamentally different from that of an adult. While adults typically view sleep as a singular “rest” state, neonatal sleep is a dynamic neurological process classified into two primary types: Rapid Eye Movement (REM), often referred to in pediatrics as “active sleep,” and Non-Rapid Eye Movement (NREM), or “quiet sleep”.
The “Active Sleep” Dominance (REM) In the initial postnatal weeks, newborns sleep approximately 16 to 18 hours per day, yet this sleep is highly fragmented into short intervals ranging from 2.5 to 4 hours.
Crucially, nearly 50% of this time is spent in active (REM) sleep—a hallmark of early brain development. During this state, you may observe:
- Rapid eye movements under the eyelids.
- Irregular breathing patterns.
- Low-level muscle twitches or “startles.”
This high level of neural activity is hypothesized to facilitate the maturation of sensory systems and the refinement of neural circuits through endogenous stimulation.
The 60-Minute Cycle Vulnerability Unlike adults, who have a sleep cycle of 90 to 110 minutes, a newborn’s total sleep cycle is roughly 40 to 60 minutes. Furthermore, while adults enter sleep through quiet NREM stages, newborns initiate sleep via REM.
The Moro Reflex Factor: Often called the “startle reflex,” this is a primitive neurological response where the infant feels as if they are falling, causing them to suddenly spread their arms. This reflex is a primary reason for awakenings in a newborn sleep schedule, especially during the transition from being held to being placed in a flat crib.
Implication for Parents: This shorter cycle means that infants pass through light sleep more frequently, significantly increasing the likelihood of arousal due to environmental “noise” (like a door closing) or internal physiological signals (like hunger or gas).
Chronobiology: Maturation of the Internal Pacemaker
One of the most distressing phenomena for new parents is “day/night confusion,” clinically known as circadian misalignment. To understand why this occurs, we must look at the Suprachiasmatic Nucleus (SCN), the body’s master clock.
The “Melatonin Gap” (0-9 Weeks) In utero, the fetus is biochemically synchronized with the mother. Maternal melatonin crosses the placenta, regulating the fetal sleep-wake cycle.
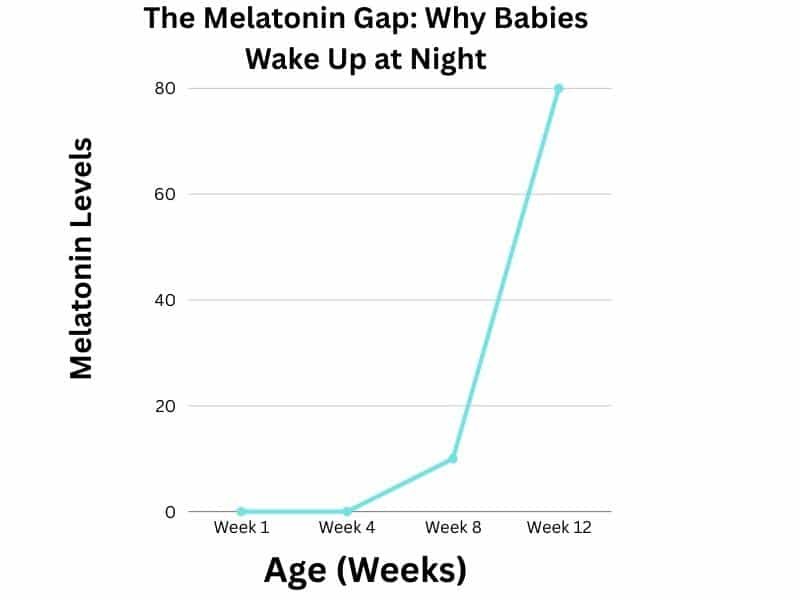
- At Birth: This supply is severed. The infant’s own pineal gland is not yet mature enough to synthesize melatonin in meaningful quantities.
- The Result: From weeks 0 to 9, the infant exists in a state of “free-running” rhythm, unrelated to the solar day. Because the circadian pacemaker is still developing, attempting to force a rigid newborn sleep schedule before this biological milestone is often counterproductive.
Research Insight (Chrononutrition): Interestingly, nature provides a temporary bridge. This concept is known as Chrononutrition: maternal breast milk produced at night contains significantly higher concentrations of melatonin than daytime milk, acting as an exogenous sleep aid for the infant. This is why “pump and dump” timing matters feeding “day milk” at night can accidentally signal the baby to wake up. Since maternal diet directly impacts milk composition and infant alertness, many parents ask about stimulants; for a full breakdown, see our Caffeine and Breastfeeding Guide.
The Role of Cortisol and Stress While melatonin (the sleep hormone) is low, cortisol (the stress/alertness hormone) functions differently in neonates. Research indicates that unlike adults, whose cortisol peaks in the morning, newborns lack a rhythmic cortisol secretion pattern until approximately 3 months of age.
Scientific Implication: You cannot “train” a biological clock that does not yet exist. Attempts to force a strict schedule before the SCN matures (around 12 weeks) are not only futile but may induce unnecessary physiological stress.
Environmental Entrainment (The Fix) Since the internal clock is immature, the infant relies on external cues, known in chronobiology as Zeitgebers (time-givers).
- Light: Exposure to natural blue-spectrum light in the morning stimulates the SCN.
- Feeding: Regular gastric emptying creates a metabolic rhythm that helps set the sleep clock.
The 2026 Safe Sleep Standards: Mitigating SIDS Risks
Safety is the most critical component of a newborn sleep schedule, and in the United States, adherence to the American Academy of Pediatrics (AAP) guidelines is the non-negotiable standard for neonatal care. The primary objective is the prevention of Sudden Infant Death Syndrome (SIDS) and accidental suffocation.
The “ABCs” of Sleep (Physiological Basis) To minimize the risk of carbon dioxide rebreathing and airway obstruction, the AAP mandates the following protocol for the first 12 months:
- A (Alone): The infant must sleep without pillows, blankets, bumpers, or stuffed animals. Soft objects pose a suffocation risk and can increase thermal insulation, leading to hyperthermia (overheating), a known SIDS risk factor. The infant should sleep in their own dedicated space (crib or bassinet) without other people, pets, or soft objects. Crucially, the AAP recommends “Room-Sharing without Bed-Sharing,” suggesting that keeping the infant’s crib in the parents’ bedroom for at least the first six months can reduce the risk of SIDS by as much as 50%. This proximity allows for rapid response to feeding cues and respiratory changes within the newborn sleep schedule.
- B (Back): The supine position (sleeping on the back) is the only safe position. Research confirms that this position stabilizes the trachea and does not increase the risk of aspiration, even in infants with reflux.
- C (Crib): The infant should sleep on a firm, non-inclined surface that meets CPSC Safety Standards. This ensures the sleeping environment is free from hazardous designs that could compromise the airway or lead to accidental entrapment.
The Danger of Inclined Sleepers & “Positional Asphyxia” Despite their popularity for soothing reflux, inclined sleepers (swings, rockers, or car seats used outside the car) are contra-indicated for routine sleep.
- The Mechanism: When an infant’s head slumps forward due to weak neck muscles, the airway can become compressed. This phenomenon, known as positional asphyxia, effectively cuts off oxygen supply silently.
- The Rule: If an infant falls asleep in a swing or car seat, they should be moved to a flat, firm surface immediately. This transition is a non-negotiable safety rule for any newborn sleep schedule.
A Note on Weighted Sleep Sacks (2026 Update) The AAP and the Centers for Disease Control (CDC) have issued warnings regarding weighted swaddles and sleep sacks. The concern is that the added weight may compress the developing thoracic cage, potentially impairing respiration and—critically—dampening the infant’s natural arousal mechanism, which is their primary defense against SIDS.
The “M-Position” and Hip Development:
While a snug swaddle can help soothe the startle reflex, it must not be restrictive to the lower body. According to the International Hip Dysplasia Institute, swaddling an infant with their legs pulled straight or pressed together can lead to hip dysplasia or dislocation. For a safe newborn sleep schedule, always ensure a “Hip-Healthy” swaddle: the baby’s legs should be able to bend up and out at the hips (the “M-position”). Avoid any sleep sacks that are tight around the thighs or knees.
The Feeding-Sleep Connection: Gastric Physiology
A common misconception among parents is that a newborn waking every two hours is a sign of a “sleep problem.” Biologically, this is a survival mechanism driven by two physiological factors: gastric capacity and metabolic rate. Therefore, the most effective newborn sleep schedule is one that evolves week-by-week, shifting from a metabolic focus to a circadian rhythm.
The “Cherry-to-Walnut” Stomach Capacity At birth, the neonatal stomach is anatomically minute, capable of holding only 5 to 7 ml (the size of a cherry). By day 10, this expands to approximately 60-80 ml (the size of a walnut).
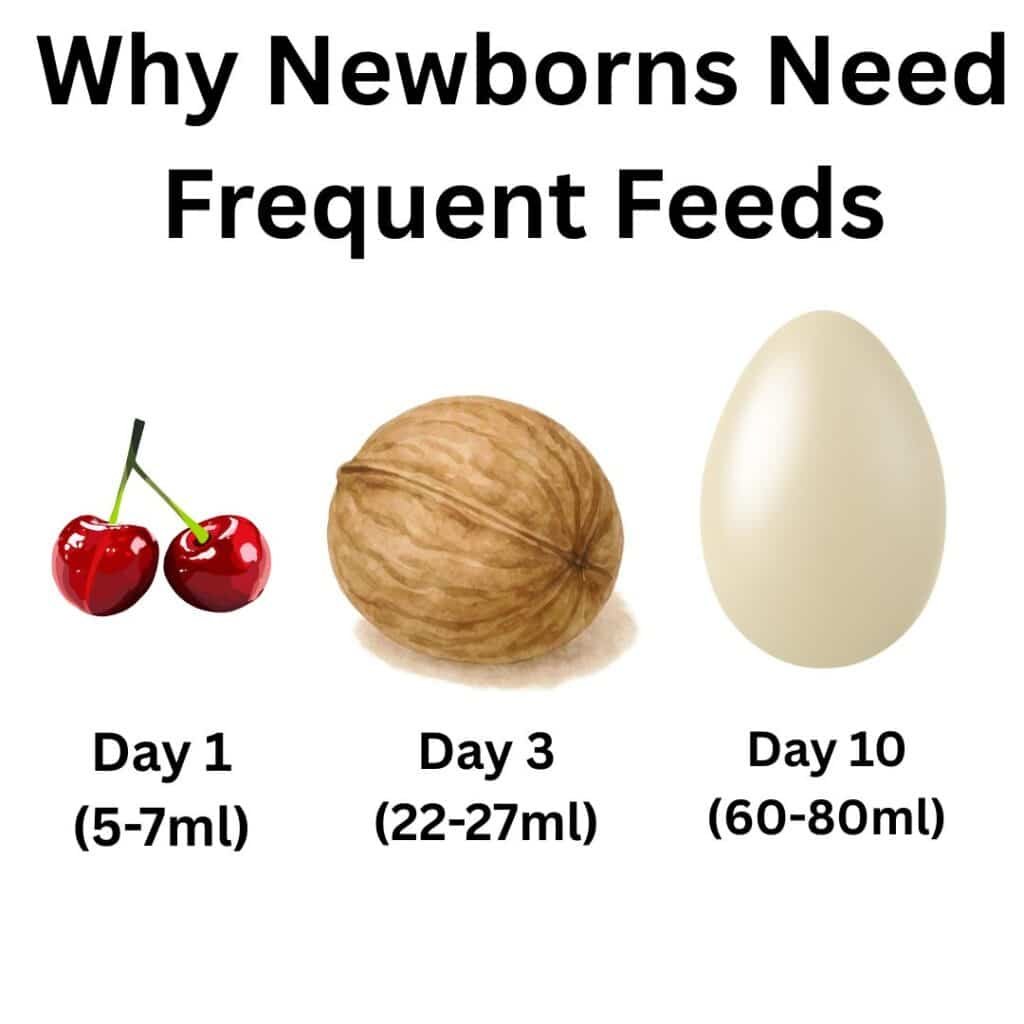
- The Consequence: The infant physically cannot consume enough calories in a single feeding to sustain a sleep period longer than 2.5 to 3 hours without risking hypoglycemia (low blood sugar).
Gastric Emptying Rates The rate at which the stomach empties dictates the sleep cycle.
- Breast Milk: Metabolized rapidly, typically emptying the stomach in 60 to 90 minutes.
- Formula: Due to the casein protein structure, formula takes longer to digest, potentially extending sleep blocks slightly, though not significantly in the first weeks.
The Role of Gastrointestinal Discomfort (Colic & Gas) A major disruptor of neonatal sleep is Aerophagia (air swallowing) during feeding. Since the infant’s digestive system is immature, trapped gas bubbles can cause distension and pain, triggering immediate arousal from sleep.
Research Note: Many parents utilize pharmacological aids to manage this discomfort. For a detailed chemical analysis of Simethicone versus Probiotics, read our scientific review on Infant Drops for Gas: Mechanism of Action.
The Physics of Gas Relief (Young-Laplace Equation):
Simethicone functions by altering surface tension. Scientifically, it follows the Young-Laplace Equation (Δp = 2γ/R), which dictates that by lowering surface tension (γ), small gas bubbles coalesce into larger ones, allowing them to be expelled more easily as flatulence. Understanding these digestion speeds helps parents set realistic expectations for a newborn sleep schedule during the first month.
The Developmental Roadmap: A Week-by-Week Guide
Below is the neurobiologically appropriate timeline for sleep maturation. Note that these are statistical averages derived from clinical data, not rigid rules. Every infant’s central nervous system matures at a slightly different velocity. The following phases outline a biologically appropriate newborn sleep schedule that respects the infant’s need for frequent feeding and sensory integration.
Phase 1: The “Free-Running” Stage (Weeks 0-4)
During this neonatal phase, the infant has no internal clock. Sleep pressure is driven entirely by Adenosine (a chemical that builds up in the brain) and hunger.
- The Goal: Survival and recovery. Do not attempt a strict schedule.
- The Science: The infant sleeps 16-18 hours but rarely for more than 2-4 hours at a time making a traditional newborn sleep schedule impossible due to the need for glucose regulation.
- Actionable Step: Focus on Day/Night differentiation to set the foundation for a future newborn sleep schedule. Morning light hits the retina and travels via the Retinohypothalamic Tract directly to the brain’s clock, signaling “Wake Up.” Keep days bright and noisy; keep nights pitch black.
External Resource: For official guidelines on safe sleep environments during this fragile stage, refer to the AAP HealthyChildren.org Safe Sleep Page.
Phase 2: The Peak of Arousal (Weeks 5-8)
This period often coincides with the peak of “PURPLE Crying” or Colic. The nervous system is becoming highly sensitive to stimuli, and digestive issues peak.
- The Challenge: Wake windows slightly increase, but the baby becomes “overtired” rapidly.
- The Research Perspective: Many parents panic, assuming their newborn sleep schedule has failed, but this regression is biologically normal.
- Internal Link: As I explain in my researcher bio, this is a developmental milestone, not a medical failure. Read more about My Research Background & Methodology to understand why we prioritize biological cues over strict schedules.
- The “Pause” Method: French pediatricians recommend waiting 3-5 minutes before responding to a cry (unless it is a hunger cry) to allow the infant to practice self-soothing (connecting sleep cycles).
Phase 3: Circadian Emergence (Weeks 9-12)
Biologically, this is the turning point. Endogenous melatonin production begins, and the cortisol rhythm stabilizes.
- The Shift: You will notice that your newborn sleep schedule becomes more predictable, with longer stretches of night sleep (4-5 hours) as the stomach capacity increases.
- Routine Implementation: Now is the time to introduce a consistent bedtime sequence (Bath > Massage > Feed > Bed). According to a study published in the Journal of Sleep Research, consistent bedtime routines reduce night wakings by 48%.
The 2026 Newborn Sleep Schedule & Architecture Data.
| Infant Age | Total Sleep (24h) | Wake Window (Max) | Number of Naps | Physiological Goal |
|---|---|---|---|---|
| 0 – 4 Weeks | 16 – 18 Hours | 45 – 60 Minutes | Variable (5-7) | Glucose Stability |
| 5 – 8 Weeks | 15 – 17 Hours | 60 – 90 Minutes | 4 – 5 Naps | Sensory Integration |
| 9 – 12 Weeks | 14 – 16 Hours | 75 – 100 Minutes | 3 – 4 Naps | Circadian Entrainment |
Watch Video Given Below: How To Put Your Baby To Sleep, According To “The Baby Whisperer”
Watch this helpful video by Insider on YouTube
The Researcher’s Verdict: Actionable Summary
Science ko daily routine mein apply karne ke liye, ye aakhri nukaat (points) yaad rakhein:
- Digestive Comfort: Agar bacha gas ki wajah se pareshan hai, toh research ke mutabiq L. reuteri strain wale probiotics simethicone drops se zyada effective sabit hue hain. Apne pediatrician se is specific strain ke baaray mein mashwara karein.
- Acoustic Environment: Sound machine ka istemal zaroori hai magar check karein ke volume 60 dB se zyada na ho aur wo crib se kam az kam 7 feet door ho taake auditory development mutasir na ho.
- Thermal Safety: Overheating se bachne ke liye TOG-rated wearable blankets ka intekhab karein. 68-72°F ke kamray ke liye 1.0 TOG rating sab se mahfooz aur scientific standard hai.
While focus is often on the baby, maternal recovery is equally vital; ensuring comfort during the transition home is essential, as discussed in our guide on Postpartum Going Home Outfits.
Conclusion: The Biological Reality
Final Thought on Your Newborn Sleep Schedule:
While the first 12 weeks are biologically demanding, remember that you are not just managing hours of rest; you are supporting the delicate maturation of your child’s brain.
The expectation that a human neonate should sleep through the night is a cultural imposition, not a biological reality. The first 12 weeks of life are defined by the maturation of the Suprachiasmatic Nucleus and the rapid expansion of gastric capacity.
By understanding the limitations of the newborn nervous system, parents can shift their goal from “training” to “supporting.” The objective in the fourth trimester is not to enforce a rigid schedule, but to facilitate the natural emergence of circadian rhythms through environmental cues—light, feeding, and safe sleep practices.
As we move toward the 4-month mark, sleep architecture will mature, allowing for independent sleep initiation. Until then, responsive parenting is the only scientific standard.
Frequently Asked Questions (Scientific Analysis)
When do newborns biologically sleep through the night?
Is “Cry It Out” (Extinction) safe for newborns?
What is the ideal room temperature for SIDS prevention?
Is white noise safe for newborns?
Hafiz Nauman Baig is a Researcher and PhD Scholar in Zoology, with a specialized focus on Biomechanics and Anatomical Data Analysis. Merging his academic expertise in biological structures with a deep background in Physical Ergonomics and strength mechanics, Nauman evaluates baby gear through a rigorous scientific lens.
Unlike standard product reviewers, he utilizes R Studio and statistical modeling to assess safety data, focusing on the physiological impact of carriers on the infant airway and the caregiver’s spine. His mission is to bridge the gap between complex biological safety standards and practical, pain-free babywearing.


