
👋 Welcome Moms & Dads!
As a PhD Researcher, my priority is your baby’s safety and your peace of mind. The insights in this guide translate complex biomechanics and strict safety standards into easy, everyday tips to help you build the perfect baby registry.
Scientific Note: This content is for informational purposes to guide your gear choices and does not constitute medical advice. Always consult your pediatrician!
Is a parent’s back aching after just ten minutes of carrying their newborn, or are the infant’s legs dangling straight down as if suspended in a parachute harness? Examining infant development through the lens of zoological science and biomechanics reveals exactly why everyday babywearing can either build a strong, healthy skeleton or inadvertently risk long-term joint deformation.
The science of how the human body moves dictates whether a simple walk to the park provides comfort or causes physical trauma to a mother’s healing postpartum body and a child’s soft cartilage. This comprehensive resource bypasses marketing terminology to focus on the science of M-position baby carrier hip health, relying strictly on physiological evidence, orthopedic safety data, and federal testing standards. The following report translates complex medical literature into simple, everyday science, explaining exactly why poor carrier design causes physical pain and how to protect an infant’s skeletal health. For a complete overview of all safety protocols, first review our foundational guide on comprehensive biomechanical and regulatory safety standards.
Comparative Specification Analysis: Fastener Material Science
While focusing on M-position baby carrier hip health is vital for orthopedic development, a baby carrier is only as safe as its weakest structural component. Federal testing under safety standards evaluates load-bearing fasteners under dynamic stress, pulling on them with intense force to simulate a bouncing toddler. The chemical composition of the plastic used in these buckles dictates whether they will hold up to everyday heavy lifting or shatter unexpectedly.
| Active Ingredient / Material | How it Works (Simple Physics) | Safety & Age Limit | FDA / Clinical Notes | Avg. Market Price (USD) |
|---|---|---|---|---|
| Acetal Homopolymer (Delrin) | Highly crystalline molecular structure creates extreme rigidity. Acts like a metal spring, snapping back into place without losing shape. | Safely supports maximum weight limits (45+ lbs). Retains extreme tensile strength (up to 10,000 psi) in sub-zero temperatures. | Preferred material for precision medical devices. Highly resistant to chemical degradation and daily wear. | Premium tier carriers ($130 – $370+). |
| Polyamide (Nylon) | Flexible and tough. Bends slightly to absorb shock rather than cracking, acting like a structural shock absorber. | Safe for standard infant limits (35 lbs) but absorbs environmental moisture, which can cause slight swelling over time. | Used heavily in soft-goods and standard outdoor gear. Fails faster under exposure to strong cleaning chemicals. | Mid-tier carriers ($60 – $120). |
| High-Density Polyethylene (HDPE) | A moisture-resistant thermoplastic that offers high impact strength but less overall stiffness than Acetal. | Safe for mid-range weights (up to 30 lbs). Better for static loads rather than dynamic, bouncing weights. | Commonly used in medical packaging and standard consumer goods. Highly resistant to chemical cleaners. | Budget-to-Mid tier ($40 – $80). |
| Standard Polypropylene (Cheap Plastic) | Basic polymer chains that lack the structural “memory” to snap back repeatedly under heavy loads. | Prone to stress-fractures under dynamic weight (e.g., a jumping toddler). High risk of mechanical failure over 20 lbs. | Often found on unregulated, uncertified counterfeit carriers originating from generic online marketplaces. | Budget / Counterfeit ($20 – $40). |
Researcher’s Takeaway: (In simple words: Cheap plastic buckles break. Only buy carriers featuring buckles made of “Delrin” (Acetal) because they possess intense structural memory. They will not snap or slip when a parent bends over to pick up a dropped toy, ensuring the baby’s weight is always securely locked in place to maintain proper M-position baby carrier hip health).
Table of Contents
Educational Narrative: The Biomechanics of Infant Carrying
To fully grasp the necessity of ergonomic baby equipment and the critical importance of M-position baby carrier hip health, one must first understand the unique zoological status of human infants:
- Evolutionary Compromise: Human babies are born highly undeveloped to allow a large brain to pass through the maternal pelvis.
- Secondary Altriciality: Compared to mammals like foals that walk within hours of birth, human infants require constant physical support.
- The “Fourth Trimester”: A baby carrier acts as an “external womb,” supporting the baby against gravity while their skeletal structure finishes forming, making M-position baby carrier hip health a daily necessity.”
The Biological Blueprint of the Infant Skeleton
When a baby is born, their skeleton is not constructed of hardened, calcified bone like that of an adult. Instead:
- Critical joints remain highly malleable and soft.
- The skeletal structure relies entirely on external support to maintain safe alignment.
The Anatomy of the Hip Socket (The Wet Clay Analogy)
The hip joint is a classic ball-and-socket mechanism, which in a newborn has specific vulnerabilities:
- The “Wet Clay” Socket: During the first six months, the hip socket (acetabulum) is primarily composed of soft, flexible cartilage, comparable to a shallow bowl made of wet clay.
- The Malleable Ball: The femoral head (the ball of the joint) rests inside this shallow bowl. Gentle, centered pressure helps carve out a deep, permanent socket.
- Hormonal Laxity: Maternal hormones that relax ligaments for childbirth also cross the placenta, leaving the infant’s ligaments incredibly loose and stretchy.
- High Risk of Slipping: Because the ‘bowl’ is shallow and ligaments are loose, the ball is at a high risk of slipping out of place, which is exactly why preserving M-position baby carrier hip health is so critical.
How Leverage Causes Dislocation
Improper positioning in a carrier can physically alter the shape of the developing joint:
- The Crowbar Effect: If legs are forced straight down and held tightly together, the long thigh bones act as rigid levers, pulling the hip ball away from the center.
- Cartilage Deformation: Constant outward pressure flattens the soft edges of the cartilage bowl, causing the ball to misshape the socket or slip out completely.
- Developmental Dysplasia of the Hip (DDH): This painful, debilitating condition is the direct result of this prolonged mechanical leverage.
- Cultural Evidence: Societies using rigid swaddling (legs strapped straight) show astronomically high DDH rates. Conversely, cultures carrying infants on the back with legs spread wide have virtually no hip dysplasia.
Decoding the M-Position Geometry
How to use this Carrier Sizing Matrix: This interactive diagnostic calculator evaluates your infant’s current age, weight, and your specific anatomical requirements (including torso length and postpartum C-section recovery) to recommend the safest ergonomic carrier style. Simply select your parameters to generate a personalized recommendation that mathematically preserves the infant’s orthopedic M-position while protecting your pelvic floor and lower back.
The biological antidote to hip dysplasia is a specific posture recognized by pediatric orthopedic specialists globally, serving as the ultimate foundation for M-position baby carrier hip health:
- It mimics the natural, instinctive clinging position of human infants.
- It supports millennia of mammalian evolutionary development.
The Cone of Stability and the Fetal Tuck
The healthiest geometric alignment for an infant’s lower body is the “Spread-Squat” or “Jockey” position:
- Optimal Angles: The baby’s hips are spread apart (abducted roughly 40 to 55 degrees) and bent upward toward the stomach (flexed 90 to 110 degrees).
- The “M” Shape: Knees are elevated slightly higher than the buttocks, with fabric supporting the entire thigh to the back of the knee joint.
- Core Principle: This visual alignment is the very foundation of M-position baby carrier hip health.
- The Cone of Stability: Biomechanical studies show this geometry places the ball of the hip squarely into the safest, most stable zone of the socket.
Ultrasound Evidence and Joint Reaction Forces
Scientific research utilizing real-time ultrasound technology provides clinical proof of this positioning:
- Medical Grade Alignment: Wide-base carriers hold hips in a position remarkably similar to the Pavlik harness (the premier medical device used by doctors to cure hip dysplasia).
- Beneficial Muscle Engagement: Wrapping legs around the parent’s torso allows the infant to gently grip with inner thigh muscles.
- Stimulating Growth: These natural gripping forces stimulate healthy cartilage growth and joint ossification (hardening into bone).
Identifying Orthopedic Safety in Consumer Products
Understanding the science of the M-position is only half the battle. Parents must also navigate a saturated, highly commercialized market of baby gear to find equipment that mechanically supports this posture and ensures true M-position baby carrier hip health.
- The Educational Authority: The International Hip Dysplasia Institute (IHDI) functions as an educational body that evaluates infant products.
- Proactive Acknowledgment: They officially acknowledge products that proactively promote healthy joint development.
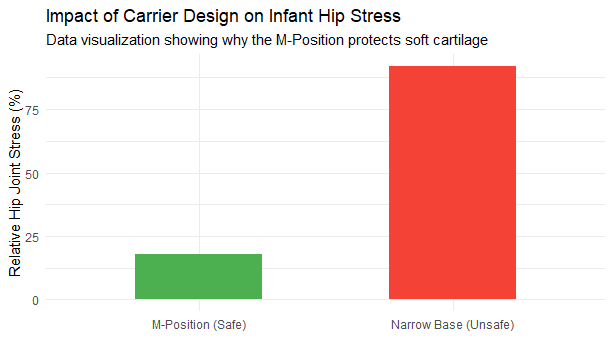
The Danger of the “Crotch Dangler” Design
The fundamental flaw of this narrow design is that it actively works against the biomechanical principles of M-position baby carrier hip health. A truly ergonomic carrier must feature a wide base of support. Narrow-based carriers—often colloquially referred to by frustrated parents in online forums as “crotch danglers”—pose significant physical risks:
- Suspended by the Groin: They fail to support the thighs, leaving the baby’s entire weight suspended solely by their groin.
- The Bicycle Seat Analogy: Imagine sitting on a narrow bicycle seat with your legs dangling freely without touching the ground for an hour. The heavy leverage placed on the hip joints would become intensely painful very rapidly.
- Concentrated Pressure: Concentrating a 15-pound infant’s entire body weight onto a surface area of just a few square inches can cause severe chafing, friction burns, and restricted blood circulation.

Figure 2: The Safe vs. Unsafe Leg Geometry Checklist. Always ensure the thigh is fully supported to the knee joint.Verifying Thigh Support and Base Width
While short-term use of narrow carriers may not independently cause dysplasia in perfectly healthy hips, their prolonged use is highly discouraged:
- Missing the Benefits: They completely lack the proactive developmental benefits of M-position baby carrier hip health.
- Exacerbating Instability: Dangling legs can rapidly worsen hidden, pre-existing joint instability.
- The Knee-to-Knee Rule: When shopping, parents must look for ‘IHDI Acknowledged’ labels, ensuring the seat is wide enough to reach the back of the baby’s knees to guarantee optimal M-position baby carrier hip health. However, because scammers often steal these logos, you must learn how to identify counterfeit CPSC compliance labels on Amazon before purchasing.
Mastering Airway Management in Fabric Devices
While M-position baby carrier hip health addresses long-term physical development, airway management addresses immediate, life-critical safety. For a complete biomechanical breakdown of how to protect your infant’s airway, we highly recommend reading our comprehensive guide on TICKS rule baby carrier safety.
- Disproportionate Anatomy: A newborn’s head is disproportionately large and heavy compared to their body.
- Undeveloped Musculature: Their cervical spine (neck) muscles are entirely undeveloped and cannot fight gravity.
The “Wet Paper Straw” Analogy for Infant Windpipes
A newborn’s trachea (windpipe) is incredibly soft and pliable:
- The Straw Effect: It is structurally comparable to a thin, wet paper straw.
- The “C-Shape” Collapse: If a carrier lacks proper back support, the heavy head inevitably slumps forward, forcing the chin down onto the chest.
- Kinking the Airway: This collapse effectively kinks the “wet paper straw,” severely restricting oxygen flow to the lungs.
- Silent Hypoxia: Because the infant lacks the muscle tone to lift their head and cannot vocalize their distress through crying, this leads to a terrifying, silent loss of oxygen.
Executing the TICKS Rule for Daily Safety
To ensure ergonomic positioning that absolutely protects the infant airway, safety experts rely on the universally recognized TICKS framework:
- (T)ight: The fabric must hold the baby firmly. Use the “Bend Test” (if you lean forward, the baby should not pull away from your body).
- (I)n View at All Times: You must be able to see the child’s nose and mouth simply by glancing downward to prevent CO2 re-breathing.
- (C)lose Enough to Kiss: Positioned high on your chest, out of the hazardous “slump zone” near the stomach.
- (K)eep Chin Off Chest: There must always be a visible gap of at least 1-2 finger widths between the baby’s chin and chest.
- (S)upported Back: The carrier must act as a rigid substitute for your hands, maintaining the spine’s natural curve.
The Human Experience: Maternal Biomechanics and Healing
A discussion of baby carrier safety is incomplete without addressing the physical reality of the adults wearing them.
Cesarean Section Recovery and Waistband Physics
Motherhood often involves recovering from major abdominal surgery (C-section), leaving the abdominal muscles and fascia severely compromised:
- Dangerous Leverage: Narrow, poorly structured carriers shift the adult’s center of gravity forward, pulling directly on the healing abdominal incision.
- The Hiking Backpack Solution: Ergonomic carriers solve this by incorporating a wide, heavily padded lumbar belt.
- Pelvic Anchoring: This belt transfers the entire gravitational load down to the wearer’s iliac crest (the strong pelvic bones), bypassing the weakened surgical site entirely.

Figure 3: Lumbar Belt Physics. Ergonomic carriers transfer the baby's weight directly to the strong pelvic bones (Iliac Crest), preventing neck and shoulder strain.The “Rib Belt Effect” for Taller Caregivers
Taller caregivers, such as fathers over six feet tall, face a unique biomechanical challenge:
- Standard Sizes Fail: “One size fits all” waistbands often fail to reach their hips due to longer torso measurements.
- The Rib Belt Effect: Instead of sitting on the hips, the belt rides up and crushes their lower ribs, causing severe discomfort and respiratory restriction.
- The Fix: Ergonomic positioning for tall parents requires adjustable panel heights and generous webbing lengths to anchor the weight safely.
The Digital Evidence Brief
To establish true analytical authority on M-position baby carrier hip health, it is necessary to move beyond generalized advice and examine the rigid legal frameworks, testing protocols, and real-world consumer data that govern the baby carrier industry.
Label Analysis: The Legal Language of Safety
Federal regulations require baby carriers sold in the United States to pass rigorous mechanical and labeling tests. Most consumer parenting blogs miss the strict, scientific exactitude required by these laws.
To understand the exact laboratory testing your gear undergoes, explore our detailed analysis of the ASTM F2236-24 baby carrier safety standards.
- The Unbounded Leg Opening Rule: The revised test utilizes a specialized 17-pound shot bag and a rigid, truncated cone measuring exactly 4.7 inches in diameter. This ensures that an infant with a smaller-than-average leg circumference cannot slip completely through the leg holes.
- ANSI Z535.4 Compliance: Warning labels must strictly follow specific formatting, signal words, and color psychology (e.g., “DANGER” in white letters on a red background) to overcome language barriers.
- The Nursing Suffocation Mandate: The new law requires explicit warning text stating that caregivers must immediately reposition the baby to a high, tight, and upright position after nursing. Leaving a baby in a loose feeding position presents an acute, rapid suffocation hazard.
Consumer Analysis: Validating Parental Pain
A deep analysis of consumer forums, such as Reddit’s babywearing communities, reveals a stark disconnect between aggressive brand marketing and the actual human experience:
- The Chafing Reality of “Crotch Danglers”: Suspending a baby entirely by their groin concentrates all gravitational force onto a highly sensitive area, causing severe chafing, red marks, and restricted circulation. Many consumer complaints regarding infant discomfort could be entirely resolved by switching to a device that actively supports proper M-position baby carrier hip health.
- The “In-Between” Size Dilemma: In poorly designed soft-structured carriers, the narrow setting is too small, but the wide setting stretches the baby’s legs into a straight line (forcing knee hyper-extension).
- The Agony of the Unstructured Waistband: If a carrier lacks a structured, rigid waistband, 100% of the infant’s weight hangs directly from the wearer’s trapezius muscles, leading to massive abandonment of babywearing due to crippling neck pain.
Video Demonstration: Protecting Infant Hip Sockets
Video 2 (Hips): “Imagine sitting on a narrow wooden barstool vs. a wide fabric hammock. Let’s look at how to properly execute a ‘Pelvic Tuck’ to protect delicate hip sockets.”
8. High-Intent FAQs: Parent’s Guide to Carrier Safety
Parents searching for safety information are often highly anxious. The following answers bypass clinical jargon to provide clear, scientifically sound reassurance:
Can a narrow baby carrier cause hip dysplasia?
Is it safe for my baby to face outward in a carrier?
Does my child still need the M-position when they are a toddler?
Are cheap internet baby carriers dangerous to use?
Can I let my baby sleep while I am wearing the carrier?
Do I really need a bulky, padded waistband on my carrier?
Should I wear my newborn while I am cooking dinner?
The Researcher’s Verdict
When evaluating the vast landscape of infant transport gear, the biological and biomechanical evidence overwhelmingly points toward a multimodal strategy that refuses to compromise on either orthopedic geometry for the child or physical sustainability for the parent. Ultimately, investing in a product that guarantees M-position baby carrier hip health is a lifelong investment in your child’s orthopedic future.
The ultimate, science-backed solution lies in selecting an IHDI-acknowledged, wide-based carrier that physically enforces the natural M-position.
- This carrier must be constructed with high-tensile Delrin fasteners that will not fail under stress.
- It must feature a broad, rigid lumbar support system to protect the wearer’s core.
Final Thought: Infant equipment is not just a fabric fashion accessory; it is a vital, weight-bearing tool designed to protect a highly malleable skeleton and a fragile airway. While protecting the skeleton is your structural priority, you must also protect your baby’s sensitive skin by verifying OEKO-TEX Standard 100 chemical limits for skin contact. Prioritize the science of how the human body moves, adhere strictly to the TICKS airway safety framework, and trust that a structurally sound, ergonomic carrier is one of the most critical investments a family can make for a child’s long-term physical foundation.
Works Cited
- Baby Carrier Safety SEO articles of phase 1.pdf
- Notice of Proposed Rulemaking: Safety Standard for Soft Infant and Toddler Carriers (CPSC)
- What Is the Difference Between Acetal Plastic and Delrin? (Emco Industrial Plastics)
- 10 Best Baby Carriers Tested (Momcozy & Babylist)
- HDPE vs. Delrin®: Material Differences and Comparisons (Xometry)
- Baby Carriers & Other Equipment (International Hip Dysplasia Institute)
- Developmental Dysplasia of the Hip – StatPearls (NCBI Bookshelf)
- ANSI Z535.4‑2023: Guide to Product Safety Signs & Labeling
About the Author: Hafiz Nauman Baig is a PhD Scholar in Zoology specializing in Fisheries at Quaid-i-Azam University. Leveraging advanced statistical data analysis in R Studio and research expertise in aquatic adaptation and oxidative stress, he provides rigorous, evidence-based safety and ergonomic evaluations for baby gear.


