👋 Welcome Moms & Dads!
As a PhD Researcher, my priority is your baby’s safety and your peace of mind. The insights in this guide translate complex biomechanics and strict safety standards into easy, everyday tips to help you build the perfect baby registry.
Scientific Note: This content is for informational purposes to guide your gear choices and does not constitute medical advice. Always consult your pediatrician!
Is your back killing you after 10 minutes of carrying your baby? Or worse, do you find yourself constantly checking your little one’s breathing, unsure if they are truly safe in that fabric sling? You are not alone. As a PhD Scholar in Zoology specializing in environmental toxicology and developmental biology, I approach babywearing not as a lifestyle trend, but as a biological necessity governed by the laws of physics. In the scientific world, we call this “Biomechanics”—simply put, the science of how your body moves and how mechanical forces interact with living tissue.
(In simple words: Babywearing isn’t just about cute fabric and fashion; it’s about physics. We use science to make sure the carrier supports your body without pain and keeps your baby breathing safely.)
When a carrier hurts your back or feels “off,” it is often a warning sign that the physics are wrong. More critically, an improperly positioned infant faces hidden, life-threatening respiratory risks. To build a complete foundation of infant carrying mechanics beyond just the TICKS rule baby carrier safety protocol, we highly recommend reviewing our comprehensive guide on biomechanical baby carrier safety standards.
⚠️ WARNING: The Danger of “Tracheal Kinking”
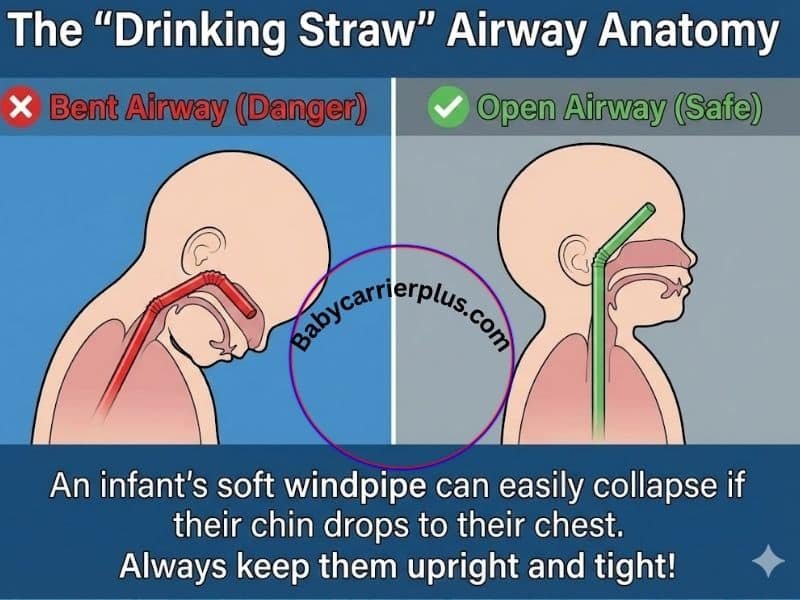
Unlike adults, newborns have a soft, undeveloped windpipe. If they slump in a carrier and their chin drops to their chest, their soft airway collapses like a bent drinking straw, silently cutting off their oxygen.
This report moves beyond marketing fluff to help you master TICKS rule baby carrier safety. I promise to explain exactly why these biomechanical failures happen and how to fix them using rigorous safety data, comparative anatomy, and the latest 2026 regulatory standards. We will translate complex physiological constraints into simple, life-saving rules, ensuring your baby’s development is supported by science, not guesswork.
How to use this Diagnostic Tool: This interactive interface functions as a sequential, real-time safety verification protocol. It breaks down the TICKS guidelines into a five-step binary assessment. You must physically evaluate your carrier and click “Yes” or “No”. If you select “No”, the tool will halt progression and provide immediate corrective measures to prevent positional asphyxia.
Comparative ‘Specification Analysis’ Table
The following table analyzes common carrier components and materials through a toxicological and biomechanical lens. It contrasts marketing terms with physical realities to aid in safety-critical decision-making.
| Active Ingredient / Material | How it Works (Simple Physics) | Safety / Age Limit | FDA / Clinical Notes | Avg. Market Price |
|---|---|---|---|---|
| Delrin® (Acetal Homopolymer) | High Tensile Strength: Acts like a “memory spring.” It resists deformation under heavy loads and snaps back without breaking. | All Ages: Essential to prevent catastrophic buckle failure. | Inert and resistant to moisture. Preferred for critical safety fasteners. | Premium Carriers: $180 – $250+ |
| Standard Polypropylene / Nylon | Moderate Tensile Strength: Softer plastics that may “creep” (stretch) over time under constant bouncing weight. | Risk: Higher failure rate in carriers for toddlers >25 lbs. | Warning: Lacks the “snap” security of acetal; check for stress fractures. | Budget Carriers: $30 – $80 |
| OEKO-TEX® Standard 100 (Class 1) | Chemical Exclusion: Fabrics tested for >1,000 harmful substances (e.g., formaldehyde). Class 1 has the strictest limits for skin contact. | Newborn Safe: Critical for infants who suck on straps. | Toxicology: Prevents exposure to carcinogens and sensitizing dyes. | Certified Carriers: $150 – $220 |
Researcher’s Takeaway: (In simple words: Cheap plastic buckles can break when you bend over. Only buy carriers with ‘Delrin’ or high-grade buckles. Similarly, ‘100% Cotton’ isn’t enough—look for the ‘OEKO-TEX Class 1’ label to ensure the strap your baby chews on doesn’t contain invisible poisons like formaldehyde.)
Table of Contents
The Biological Imperative: Understanding Infant Physiology
To truly understand TICKS rule baby carrier safety, we must first understand the organism we are carrying. Human infants are biological anomalies. Their skeletal development and respiratory systems are uniquely fragile at birth.
Secondary Altriciality: Why Humans Are “Fetuses Outside the Womb”
In the field of zoology, mammals are generally classified as precocial (foals or calves born ready to run) or altricial (kittens born blind and helpless). Human infants represent a unique paradox known as “secondary altriciality.” Because humans evolved to walk upright (narrowing the pelvis) while developing massive brains, babies must be born effectively 9 to 12 months “early” relative to their brain growth trajectory.
(In simple words: Human babies are born before their bodies are fully developed so their large heads can fit through the birth canal. Your baby carrier essentially needs to act like an external womb for the first few months to do the work their muscles cannot yet do.). Therefore, implementing TICKS rule baby carrier safety from day one is a non-negotiable step to protect this fragile physical development.”
The Primate Clinging Model & Spinal Ontogeny
An adult human spine has an “S” shape that acts as a heavy-duty spring. A newborn spine, however, has only one curve: a total kyphosis, or “C-Curve”. Safety requires preserving this natural C-curve during the first year of life.
⚠️ WARNING: The Danger of Stiff Carriers A carrier with a rigid backboard that forces the baby’s spine perfectly straight places dangerous stress on their developing vertebrae. Your carrier must be soft enough to mold to their natural “C” shape, supporting their back like a firm bandage.
The Biomechanics of Airway Safety
While hip health is a long-term orthopedic concern, airway compromise is an immediate, life-threatening event. This is why TICKS rule baby carrier safety exists.
The “Drinking Straw” Analogy: Tracheomalacia
The infant trachea (windpipe) is not a rigid, calcified tube like an adult’s. It is composed of soft, pliable cartilage rings—a condition called tracheomalacia.
(In simple words: Think of an adult’s windpipe like a stiff garden hose, but a baby’s windpipe is like a thin plastic drinking straw. If you bend a straw, the air stops. If a baby’s chin drops to their chest, their “straw” kinks and they stop breathing.)
This phenomenon is governed by physical laws of airflow resistance. Even a slight kink results in a massive increase in the work required to breathe, leading to rapid exhaustion for a newborn.
Silent Hypoxia: The Invisible Threat
When an adult’s airway is blocked, we gag, choke, and flail. Infants, however, often experience Silent Hypoxia. When oxygen drops, their physiological response is to become lethargic and sleepy to conserve energy.
⚠️ WARNING: Don’t Mistake Silence for Sleep Parents often feel their baby go quiet and limp, mistaking this oxygen deprivation for a “good nap.” If your baby’s head is slumped forward, gravity will pull their heavy head further down, making the kink in their airway even tighter. You must actively check their position, not just listen for crying! To prevent this hidden danger of silent hypoxia, consistently applying the TICKS rule baby carrier safety guidelines is your most effective defense.
Carbon Dioxide Rebreathing
Another invisible risk is rebreathing. Humans exhale Carbon Dioxide (CO2). If an infant’s face is pressed against fabric, the parent’s body, or buried inside a thick winter coat, the air around their nose and mouth becomes stagnant.
(In simple words: If your baby’s face is covered by the carrier’s hood or your jacket, they will breathe in their own exhaust fumes (CO2). This acts like a sedative, putting them into a dangerously deep sleep where they cannot wake up if they stop breathing. Always keep their face in view!)
Decoding the TICKS Rule: A Mechanical Breakdown
The TICKS rule baby carrier safety protocol is not just a catchy mnemonic for tired parents; it is a rigorous biomechanical checklist designed by safety experts to counteract the specific risks of infant anatomy.
(T)ight: Stabilizing the Center of Gravity
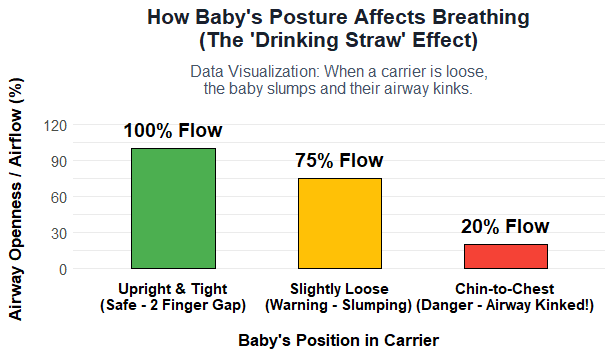
Rule: The carrier must be tight enough to hug the baby close to you. Biomechanics: Loose fabric allows gravity to act on the baby’s mass independent of the wearer. Because the baby is top-heavy, they slump. This slump creates a “C-shape” torso collapse, mechanically forcing the chin down onto the chest and kinking the airway.
(In simple words: If the carrier is loose, your baby will sag down like a sack of potatoes. This sagging bends their neck forward and closes their windpipe. A tight carrier acts like a splint, holding their back straight so they can breathe.)
Warning: Cheap imitation carriers use weak fabrics that quickly stretch out and fail this crucial tightness test. Always ensure your gear is authentic by learning how to identify counterfeit CPSC compliance labels on Amazon.
(I)n View at All Times: Visual Monitoring
Rule: You should always be able to see the baby’s face by glancing down. Biomechanics: Ensuring the face is not covered prevents the formation of CO2 pockets (rebreathing). Fluid dynamics dictate that airflow requires a clear path; fabric barriers create stagnation zones.
⚠️ WARNING: The “Silent” Danger A baby lacking oxygen will not always gasp or cry. They often just go quietly to sleep. Because they are silent, visual confirmation is the only reliable monitoring method. If their face is hidden under a hood or your jacket, you will miss the early warning signs of low oxygen (like blue lips or pale skin).
(C)lose Enough to Kiss: Anthropometrics
Rule: The baby’s head should be close enough to kiss. Biomechanics: Carrying the baby high on the chest (above your center of gravity) transfers weight efficiently into your hips. Carrying the baby too low drags on your trapezius muscles and increases lumbar torque (lower back pain).
(In simple words: If the baby is sitting on your belly instead of high on your chest, your lower back has to do all the heavy lifting. Wear the belt high on your natural waist to save your back!)
(K)eep Chin Off Chest: Maintaining Airway Patency
Rule: Ensure a gap of at least 1-2 finger widths between the baby’s chin and their chest. Biomechanics: This position maintains the head in a neutral alignment (the “sniffing position”). Anatomically, this straightens the trachea, pulling the tongue forward and ensuring the maximum diameter of the airway is maintained.
Video Guide: Watch a practical demonstration of the TICKS Rule to protect your baby’s airway. (Courtesy of Sweet Dreamers on YouTube)
(S)upported Back: Preventing Axial Loading
Rule: The carrier must support the natural curve of the back. Biomechanics: If the back is not supported, the baby’s vertebrae stack vertically on top of each other. The infant spine cannot handle this axial load.
For authoritative guidance on preventing sleep-related hazards and airway compromise, parents should consult the official Lullaby Trust sling safety guidelines, which serve as a critical reference for mastering TICKS rule baby carrier safety.
Regulatory Safety Standards: 2026 Landscape
Safety is no longer just about good intentions; it is about compliance with rigorous federal law (16 CFR Part 1226). When ensuring TICKS rule baby carrier safety, it is equally vital to verify that your gear meets the latestConsumer Product Safety Commission (CPSC) federal regulationsfor structural integrity.
ASTM F2236-24 Compliance & Buckle Integrity
High-quality carriers use primary buckles made from Delrin® (Acetal). Delrin has “memory”—it can bend under stress and snap back to its original shape. Generic carriers often use cheap plastics that suffer from “creep”—they slowly stretch and deform under constant load. While mastering TICKS rule baby carrier safety is crucial for daily use, it is equally important to understand the manufacturing side by reading our deep dive into the ASTM F2236-24 baby carrier safety standards.
(In simple words: Not all plastic clips are the same. A cheap clip from an unbranded Amazon carrier can literally snap in half while you are walking because the plastic is brittle. Only trust carriers that have passed the ASTM F2236-24 safety tests.)
⚠️ WARNING: Breastfeeding in a Carrier The 2026 regulations require a specific warning about nursing. When you loosen the carrier to breastfeed, the baby drops low and their face presses into your chest. You must immediately pull them back up to a “high and tight” position the second they finish eating. Never let a baby sleep in the lowered nursing position!
Orthopedic Mechanics: The Hip Health Mandate
While airway safety is measured in minutes, orthopedic safety is measured in years. The hip is a ball-and-socket joint. In a newborn, the socket is a shallow cup made of soft cartilage. To learn exactly how to protect this developing joint, read our definitive guide on maintaining the orthopedic M-Position to prevent dysplasia.
The “Bookshelf” Analogy: Why Narrow Bases Fail
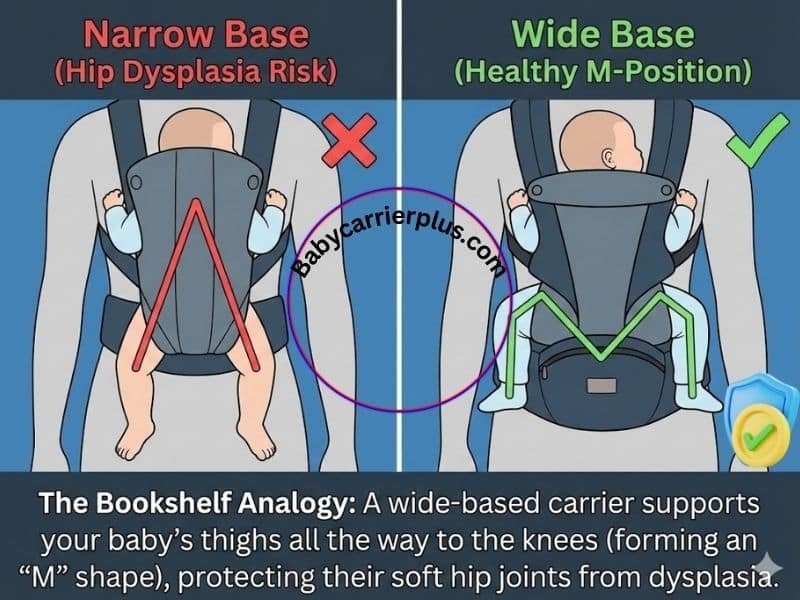
(In simple words: Think of your baby’s bottom as a heavy book. A narrow carrier is like a tiny shelf—the book is unstable and the baby’s legs dangle straight down. This dangling pulls the leg bone out of the hip socket, causing Hip Dysplasia. A good carrier is a wide shelf that supports their legs all the way to the knees, making an “M” shape.)
By tucking the pelvis and lifting the knees (the M-Position), you lock the baby onto the ‘shelf’ of the carrier. The mechanical forces push the ball bone deep into the hip socket, actually helping the hips grow stronger! If you struggle with maintaining the correct M-Position or experience lumbar discomfort even while practicing TICKS rule baby carrier safety, exploring a structured option like the Tushbaby hip seat can significantly relieve mom’s back pain.
Material Science & Toxicology: The Hidden Chemistry
Infants explore the world with their mouths. Carrier straps, which sit right next to a baby’s face, are frequently sucked, chewed, and drooled on.
The Oral Vector & OEKO-TEX
Textiles can contain invisible chemical residues like formaldehyde (used in “wrinkle-free” fabric) or heavy metals in cheap dyes.
(In simple words: Because your baby will definitely chew on the carrier straps, the fabric needs to be as safe as food. Look for the “OEKO-TEX Standard 100” label. It proves the fabric has been scientifically tested and is completely free from invisible toxic chemicals.). Even when evaluating these chemical risks, a parent’s primary focus should always return to the mechanical principles of TICKS rule baby carrier safety. To understand exactly how these invisible chemicals affect your baby’s skin, read our complete guide on verifying OEKO-TEX Standard 100 chemical limits for skin contact.
Advanced Clinical Babywearing Considerations
While the TICKS rule provides a foundational safety framework, real-world babywearing often intersects with complex physiological and environmental variables. Navigating these scenarios requires an advanced understanding of biomechanics and maternal health.
Biomechanical Management of Post-Cesarean Section and Pelvic Floor
Following a Cesarean delivery, clinical consensus dictates delaying the use of heavy, structured carriers for a minimum of four to six weeks postpartum, contingent upon medical clearance. Traditional soft-structured carriers (SSCs) feature rigid lumbar belts that frequently intersect directly with the lower abdominal surgical site, inducing severe trauma and impeding fascial healing. To bypass the abdominal quadrant, postpartum caregivers are strongly advised to utilize apron-style carriers, woven wraps, or ring slings. Furthermore, to protect the recovering pelvic floor, caregivers must maintain a neutral spinal column and integrate “360-degree diaphragmatic breathing” to ensure the mechanical load is absorbed by the deep core rather than forcing downward pressure onto weakened pelvic musculature.
Gravity-Assisted Interventions for GERD (Reflux)
Babywearing operates as a highly effective, non-pharmacological clinical intervention for the daily management of Gastroesophageal Reflux Disease (GERD). Securing the infant in a continuous vertical position utilizes gravitational force to actively retain milk and highly acidic gastric contents within the stomach cavity, drastically minimizing painful regurgitation. However, caregivers must meticulously avoid introducing iatrogenic mechanical errors. The carrier must not apply excessive compressive force to the infant’s abdominal cavity, as this extrinsic pressure can inadvertently mimic a pumping action, forcing gastric contents forcefully upward.
Thermodynamics and the Hidden Lethality of Winter Outerwear
The integration of highly insulative, bulky outerwear—specifically infant snowsuits or heavy puffers—within the restricted environment of the carrier introduces severe safety hazards. The mechanical tension required to satisfy the “Tight” requirement of the TICKS framework rapidly compresses the trapped air out of the snowsuit’s fibers. This creates hidden spatial voids and latent slack, allowing the infant to slump downward and immediately inducing perilous chin-to-chest flexion. To maintain structural safety, infants should be dressed in thin, highly breathable, moisture-wicking base layers, while the adult utilizes a specialized babywearing jacket or coat extender that envelops both the adult and the carrier system.
The Complex Spatial Geometry of Tandem Babywearing
Tandem babywearing—securing two infants to a single adult torso—amplifies both the physical load on the caregiver and the spatial complexities of airway monitoring. Twins must never share a single pouch or sling cavity, as the proximity allows their bodies to press together, creating profound mutual suffocation and carbon dioxide (CO2) rebreathing hazards. Specialized wraps engineered to preserve distinct, anatomically separate airways for each infant must be used. If utilizing a front-and-back tandem configuration, safety protocols dictate that the dorsally (back) positioned infant must possess robust, independent head, neck, and trunk control—a physiological milestone rarely achieved prior to six months of age.
Conclusion: The Scientist Parent
Babywearing is a biomechanical partnership. It provides the warmth, movement, and psychological security that a human infant craves. However, this partnership relies on you acting as their “external spine.”
By adhering to the TICKS rule baby carrier safety checklist, you are actively maintaining the structural integrity of your baby’s airway against the forces of gravity.
Final Thought: Don’t guess. Test.
- Bend Test for the airway (Is it Tight?).
- Knees-High Check for the hips (M-Position).
- Fabric Check for the chemicals (OEKO-TEX).
Your baby’s airway is as fragile as a straw—keep it straight, keep it open, and keep them close enough to kiss. Safety is the ultimate luxury. While TICKS rule baby carrier safety protects your infant’s airway, you must also protect their joints by following the International Hip Dysplasia Institute (IHDI) recommendationsfor the ergonomic M-Position.
Expert-Verified FAQs: Airway Safety & Clinical Protocols
Can my baby suffocate in a carrier?
Yes, because their windpipe is soft like a straw. If their chin touches their chest, it can close the airway. You must always keep their face visible and chin up.
Is it safe to let my baby sleep in the carrier?
Yes, but only if they are upright and you can see their face. Never let them sleep with their face pressed against your chest or completely covered by a thick fabric hood, as this stops fresh air from getting in.
How do I know if my baby’s carrier is tight enough?
Use the “Bend Test.” While supporting the back of your baby’s head with your hand, gently lean forward. Your baby’s torso should not pull away from your body. If they sag forward, the carrier is too loose.
Are cheap generic carriers on Amazon safe?
Often No, because many skip important federal safety tests. Look for a “CPC” certificate or brands that mention “ASTM F2236 compliance” to ensure the buckles won’t shatter under your baby’s weight.
Is it physiologically safe to carry my infant facing outward (world-facing)?
An infant must never be worn facing outward until they have complete, unassisted neck and trunk control (usually 4 to 6 months). Facing outward flattens their natural spinal curve and increases the risk of hip dysplasia. When permitted, it should be strictly limited to brief 20-minute intervals.
How soon after birth can I begin wearing my baby?
For healthy, full-term infants meeting the minimum weight requirement (typically 7-8 lbs), babywearing can commence almost immediately postpartum. Unstructured carriers like stretchy wraps or ring slings are medically preferred for neonates over stiff structured carriers.
Can I safely breastfeed my baby while they are secured in the carrier?
Yes, but it requires hyper-vigilance. You must continuously monitor their airway. The exact moment they finish feeding or fall asleep, you must immediately reposition them high on your chest and retighten the carrier to prevent positional asphyxia.
Why does my carrier state a max weight limit of 45 lbs, but feels unsafe with a 20 lb infant?
Manufacturer weight limits primarily reflect industrial stress testing of buckles and seams, not ergonomic comfort or physiological safety. As a baby grows, their center of mass shifts. If the carrier lacks sufficient knee-to-knee support or causes you back pain, it has outlived its functional utility.
Why are horizontal “cradle carries” or “bag slings” considered highly dangerous?
Bag-style slings force the infant into a deeply curled ‘C’ shape, aggressively pushing their chin to their chest. This creates the exact lethal conditions that induce rapid positional asphyxia. International safety experts strongly advise against horizontal carrying, advocating exclusively for upright vertical positioning.
About the Author: Hafiz Nauman Baig is a PhD Scholar in Zoology specializing in Fisheries at Quaid-i-Azam University. Leveraging advanced statistical data analysis in R Studio and research expertise in aquatic adaptation and oxidative stress, he provides rigorous, evidence-based safety and ergonomic evaluations for baby gear.