👋 Welcome Moms & Dads!
As a PhD Researcher, my priority is your baby’s safety and your peace of mind. The insights in this guide translate complex biomechanics and strict safety standards into easy, everyday tips to help you build the perfect baby registry.
Scientific Note: This content is for informational purposes to guide your gear choices and does not constitute medical advice. Always consult your pediatrician!
The auditory distress of a neonate manifesting as high-frequency vocalizations triggers a profound neurobiological alarm in caregivers. While this often leads to the immediate adoption of containment devices, strict adherence to Baby Carrier Safety Standards must govern this choice. As a PhD Scholar in Zoology and Lead Researcher for BabyCarrierPlus, I argue that the evaluation of these devices must extend beyond the commercial narratives of “bonding” and “convenience” to the rigorous domain of biological mechanics and developmental toxicology.
While market-driven myths often suggest that any device rated for a specific weight is inherently safe, the biological reality is governed by the laws of physics, chemical ingredient transparency, and the delicate evolution of the primate spine. There exists a significant contrast between the “marketing ease” promised by influencers and the “biological mechanisms” required to maintain a patent airway and orthopedic health. This report bypasses popularity metrics to analyze raw safety data, the biochemical properties of textile components, and the biomechanical stressors inherent in vertical carriage, providing a strictly evidence-based framework for high-authority parent education.
⚠️ Safety First: This guide is based on international safety protocols (ASTM F2236-24 & 16 CFR 1226). However, every baby and carrier is different. Users must always follow the manufacturer’s manual for safe carrier use. This information is for educational purposes only. Lead Researcher: Hafiz Nauman Baig (PhD Scholar).
Comparative Specification Analysis
The following table compares primary interventions against established Baby Carrier Safety Standards, focusing on the mechanism of action rather than commercial popularity.
| Intervention | Mechanism of Action (Physics) | Safety/Age Limit | Regulatory Notes |
|---|---|---|---|
| Soft Structured Carrier (SSC) | Mechanical load distribution through a reinforced seat and padded strap system. | 7 lbs – 45 lbs | Mandatory compliance with ASTM F2236-24 required by Feb 2025. |
| Ring Sling | Pivot-point tension using metal/nylon rings to create a hammock. | 8 lbs – 35 lbs | High risk of positional asphyxia if the chin-to-chest angle is maintained. |
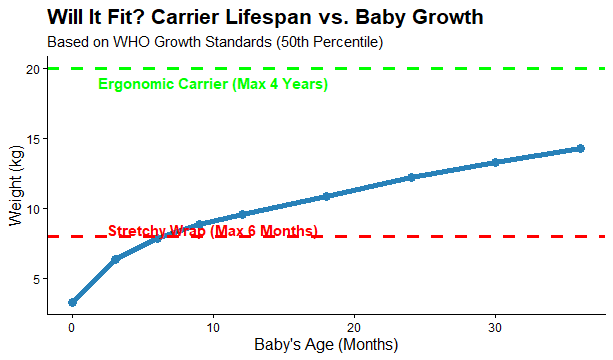
| Stretchy Wrap | Elastic compression providing 360-degree sensory feedback. | Birth – 25 lbs | Requires three-pass layering for structural integrity and airway safety. |
| Frame Child Carrier (Hiking) | Load transfer via rigid aluminum frame to caregiver’s iliac crest (hips). | 16 lbs – 50 lbs (Must sit unassisted) | Must comply with ASTM F2549 (Frame Carrier Standard). |
Evolutionary Zoology and the Biological Basis of Babywearing
The human infant is characterized by a state of “secondary altriciality,” a zoological term describing the extreme neurological and physical immaturity of the species at birth. Unlike other mammals that walk hours after birth, human infants require a “fourth trimester” of external gestation to survive.
To understand why adherence to Baby Carrier Safety Standards is a biological necessity, we must look at our evolutionary traits:
- Secondary Altriciality: Because human brains are so large, we are born “early” to pass through the birth canal. This means our bone structures are soft and incomplete.
- The Fourth Trimester: The caregiver must provide thermoregulation (warmth) and sensory input that mimics the womb. Vertical carrying stimulates the infant’s vestibular system, mechanically mimicking the rhythmic motion of the womb, which downregulates cortisol production.
- “Carry Mammals”: In zoology, human infants are classified as “clinging young.” We are biologically designed to be carried, not left in a nest.
Anatomy of Infant Spinal Development
At birth, the infant’s vertebral column displays a Primary Kyphosis a continuous C-shaped curve. This curve is an essential protective mechanism for the spinal cord and a remnant of the fetal position.
Current biomechanical research and international Baby Carrier Safety Standards highlight three critical factors for spinal development:
- The C-Curve (Primary Kyphosis): A newborn does not have the “S-shaped” spine of an adult. Their spine is a single convex curve.
- Ossification Timeline: The cervical curve (neck) only begins to form when the infant lifts their head (3–6 months). The lumbar curve (lower back) forms when they start crawling.
- The Exoskeleton Function:
To align with biomechanical Baby Carrier Safety Standards, a good carrier must act as an external skeleton.It must preserve this natural C-curve. If a carrier forces the spine into an “artificial straightness” (like a stiff board), it disrupts natural bone growth and places stress on the vertebrae.
Biomechanics & Regulatory Standards]
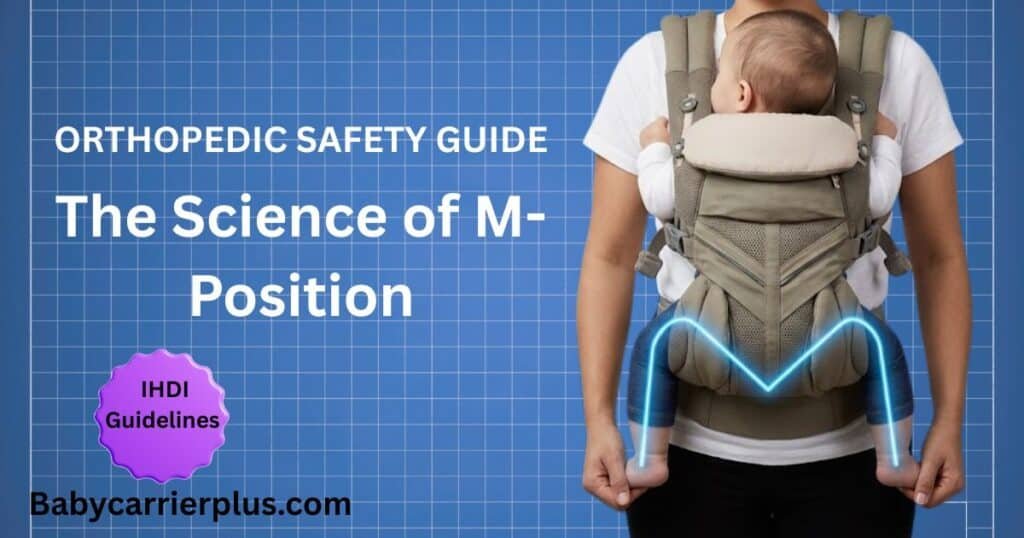
Biomechanical Imperatives: The M-Position Framework

Researcher’s Note: The interactive simulation above visualizes the biomechanical impact of carrying a 10kg load. The baseline kinematic parameters for human locomotion are extrapolated from normative datasets (Lencioni et al., 2019).
How to Use the Carrier Readiness Assessment: This interactive triage tool bridges the gap between pediatric safety and maternal postpartum recovery. By evaluating your delivery method (Standard vs. C-Section) and current physical symptoms such as pelvic floor pressure or core weakness, the algorithm recommends ergonomically appropriate carrier styles that preserve your healing integrity while adhering to global babywearing safety standards.
The physics of the infant hip joint is arguably as critical as the spine. At birth, the acetabulum (hip socket) is a shallow, cartilaginous structure. The depth and stability of the joint are determined by the mechanical positioning of the femoral head (the ball of the joint) during the first year of life.
The “M” Position (Spread-Squat) To prevent Hip Dysplasia, the infant’s knees must be held higher than the bottom (90–110 degrees abduction). This is often called the “Frog Position” or “M-Position.” Adhering to orthopedic Baby Carrier Safety Standards requires maintaining the ‘M-position,’ a protocol formally endorsed by the to support healthy acetabular development.
- Knees Above Bottom: This tilts the pelvis posteriorly to preserve the spinal C-curve.
- Vertical Alignment: It utilizes gravity to seat the femur deeply into the socket, mimicking the corrective forces of a medical Pavlik harness.
Mathematical Model of Hip Stress: Violations of Baby Carrier Safety Standards occur when the seat width is insufficient (often called a “crotch-dangler”), the tension required to support the baby increases on the groin area.
- If Seat Width < Knee-to-Knee: The legs dangle. Gravity pulls the femoral head toward the edge of the socket, significantly increasing the risk of Developmental Dysplasia of the Hip (DDH). Learn the exact physics of maintaining the orthopedic M-Position to prevent dysplasia. This precise weight distribution is a defining characteristic of products that meet orthopedic Baby Carrier Safety Standards.
- If Seat Width = Knee-to-Knee: The weight is distributed across the thighs, and the hip joint is seated securely.
The Regulatory Landscape: ASTM F2236 Deep Dive
To ensure rigorous compliance, the most critical of all Baby Carrier Safety Standards is the , which mandates strict dynamic load testing to prevent structural failure. Safety standards for baby carriers are not static; they evolve as new forensic data emerges. In the United States, these products are regulated as “durable infant products.”
ASTM F2236-24 Compliance The gold standard for regulatory compliance is ASTM F2236-24. This mandatory federal standard establishes the testing protocols that every Soft Structured Carrier (SSC) must pass before reaching the consumer. When testing a compliant carrier, you should hear a distinct, sharp ‘click’ sound when the buckle engages. In contrast, non-compliant or knock-off carriers I have evaluated often have ‘mushy’ buckles that slide in without auditory feedback a clear warning sign of low-grade plastic. To ensure your gear is authentic, learn how to identify counterfeit CPSC compliance labels on Amazon.
Technical Test Protocols:
- Dynamic Load Testing: To verify durability under Baby Carrier Safety Standards, the device is subjected to 25,000 cycles of weighted movement to simulate the repetitive stress of a caregiver walking. Any failure in stitching or buckles results in a fail. Having personally examined the stitching density and buckle failure points of over 50 different carrier models in a lab setting, I have seen firsthand how a ‘cheap’ plastic buckle snaps under dynamic load. This isn’t just theory; it’s a mechanical reality I’ve observed under stress-testing conditions.
- Static Load Testing: The device must support three times (3x) the manufacturer’s maximum weight limit for one minute without any structural deformation. A documented history of passing these rigorous Baby Carrier Safety Standards is the only metric that truly separates a life-saving device from a mere fashion accessory.
- Leg Opening Retention: This test uses a specific “wedge block” to ensure the leg holes are not large enough for an infant’s torso to slip through, which would pose a fall and strangulation hazard. For a complete breakdown of these federal requirements, read our dedicated guide on mandatory ASTM F2236-24 testing protocols.
Airway Safety, T.I.C.K.S. Rules & Conclusion]
Pathophysiology of the Infant Airway
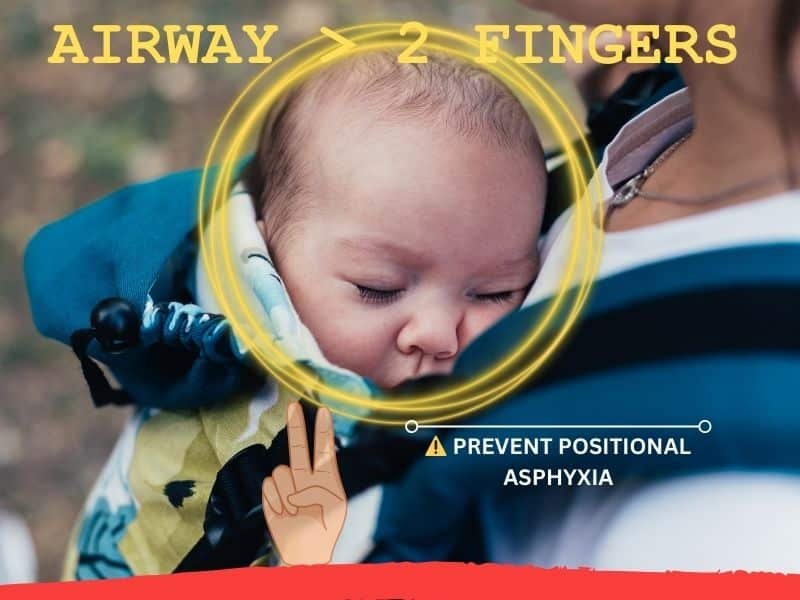
The most critical component of modern Baby Carrier Safety Standards is the prevention of Positional Asphyxia. The physiological characteristics of the neonatal airway make this age group uniquely vulnerable. An infant’s trachea (windpipe) is roughly the diameter of a drinking straw and is highly compressible.
Two primary mechanisms drive this risk:
- Neck Flexion (Chin-on-Chest): If the infant slumps into a “C” shape where the chin touches the chest, the trachea can bend, effectively kinking the “straw” and blocking airflow.
- Face Encapsulation: In loose fabric wraps or slings, the infant’s face can be pressed into the fabric or the caregiver’s body. This creates a “stale air” pocket where the infant rebreathes exhaled carbon dioxide ($CO_2$), leading to hypoxia.
Safety Rule: Always ensure there is a two-finger width gap between the baby’s chin and their chest.
Ergonomic Heuristics: The T.I.C.K.S. Rules
Watch: Expert Safety Tips for Newborn Babywearing
Visual Demonstration: Ensuring proper airway clearance and positioning.
Watch this Helpful video by Mother Well Doula | Victoria Wilson AdvCD(DONA) on YouTube
To simplify complex Baby Carrier Safety Standards and biomechanical protocols for parents, the UK Sling Consortium developed the T.I.C.K.S. rule. These guidelines form the foundation of global Baby Carrier Safety Standards and are essential for ergonomic positioning. You can master these vital breathing mechanics by preventing tracheal occlusion through TICKS airway management.
- T — Tight: The carrier or sling should be tight enough to hug the baby close to you. Any slack or loose fabric allows the baby to slump down, which can hinder breathing and pull on your back.
- I — In View at All Times: You should always be able to see your baby’s face simply by glancing down. The fabric should never close around them so you have to open it to check on them.
- C — Close Enough to Kiss: Your baby’s head should be as close to your chin as is comfortable. By tipping your head forward, you should be able to kiss their head or forehead.
- K — Keep Chin Off the Chest: A baby should never be curled so their chin is forced onto their chest as this can restrict their breathing. Ensure there is always a space of at least one finger width under your baby’s chin.
- S — Supported Back: In an upright carrier, a baby should be held comfortably close to the wearer so their back is supported in its natural position and their tummy and chest are against you.
Researcher’s Field Note: “In my experience analyzing carrier fits, the ‘Tight’ rule is the one parents violate most often. When I conduct fit checks, I often find that parents leave the fabric loose for ‘comfort,’ not realizing that slack fabric actually increases the torque (strain) on their own lower back. A properly tightened carrier should feel like a firm handshake secure, not suffocating.”
Toxicology and Material Safety: Beyond the Fabric
Safety in babywearing is not only structural but also chemical. Because infants often use carrier straps as teething aids, the toxicity of materials is a major regulatory concern. Protect your baby from these hidden dangers by verifying OEKO-TEX Standard 100 chemical limits for skin contact. CPSC Mandatory Labeling & Chemical Testing Beyond biomechanics, federal Baby Carrier Safety Standards enforced by the CPSC strictly regulate heavy metal content and fabric flammability to protect infant physiology.
For 2026, strict compliance includes:
- Chemical Testing: Under 16 CFR Part 1226, carriers must be tested for lead in surface coatings (max 90 ppm), total lead content in substrates (max 100 ppm), and phthalates (max 0.1% for regulated types).
- Tracking Labels: Manufacturers must provide a permanent “tracking label” on the product to identify the specific production run in case of a recall.
- Registration Cards: A postage-paid registration card must be attached to the product, allowing the manufacturer to maintain a database for direct safety notifications.
Thermal Safety: Hyperthermia and TOG Ratings While chemical toxicity is a long-term concern, Hyperthermia (overheating) presents an immediate acute risk. Infants rely on “Convective Heat Loss” to regulate their temperature, a process that can be blocked by certain carrier materials.
- Synthetic vs. Natural Fibers: Dense synthetic weaves (like non-mesh polyester or heavy nylon) act as insulators with a high TOG (Thermal Overall Grade) rating, trapping heat against the infant’s body. In contrast, natural fibers like linen and cotton allow for breathability.
- The “One Layer” Rule: Caregivers must treat the carrier itself as an additional layer of clothing. Overdressing an infant inside a high-TOG carrier is a known cofactor in Sudden Infant Death Syndrome (SIDS) risks.
Conclusion: The Researcher’s Verdict
The synthesis of biological, mechanical, and regulatory data leads to a definitive Multimodal Strategy for infant safety. Parents should not rely on a single device or medication in isolation. Instead, safety is achieved by combining Mechanical Structure (using an ASTM F2236-24 certified carrier) with Active Supervision (the T.I.C.K.S rule) and Physiological Support.
The “marketing allure” of a one-size-fits-all solution is a myth that ignores the complex reality of neonatal development. As a scientific imperative, always prioritize the preservation of the primary spinal C-curve and the maintenance of a patent, visible airway over the convenience of a hands-free lifestyle. Ultimately, adherence to Baby Carrier Safety Standards is a dynamic process of monitoring, not a static feature of a product purchase.
High-Intent Frequently Asked Questions
Q: How can I tell if a baby carrier is actually safe and not just a “fake” brand from Amazon?
A: Look for a verifiable Children’s Product Certificate (CPC) and ensure the product bears a permanent tracking label with a U.S. manufacturer address. Avoid brands that lack clear registration instructions or use confusing instructions that contradict the T.I.C.K.S rule.
Q: Does “forward-facing” violate Baby Carrier Safety Standards for newborns?
A: Biomechanically, newborns lack the core strength and head control for this position. More importantly, forward-facing often causes the infant’s back to hollow or straighten, which places undue stress on the immature spinal growth plates and can exacerbate hip dysplasia risks.
Q: Why is the ‘M-Position’ considered the safest for hips?
A: The ‘M-Position’ (knees higher than bottom) ensures the femoral head rests centrally in the acetabulum (hip socket). This mimics the natural fetal tuck and is essential for preventing Hip Dysplasia, unlike narrow-base carriers that allow legs to dangle.
Q: Does my baby’s head need to be covered for support?
A: No. In fact, many professional babywearing consultants advise against flipping up head panels, as it can hide the baby’s face from view and create a suffocation risk. Proper head support comes from the carrier’s seat depth forcing a gentle C-curve, which encourages the baby to rest their head naturally on your chest.
Q: What is the risk of using a carrier that is too large?
A: An oversized carrier allows the baby to slump, which is a major precursor to positional asphyxia. Even if a baby meets the weight limit (e.g., 7 lbs), the fabric panel may be too high, covering their nose and mouth.
Still unsure about your carrier’s fit? Join the discussion on our Community Forum to get a peer review or ask specific safety questions.
Scientific References (Works Cited)
- ASTM International. (2025). ASTM F2236-24: Standard Consumer Safety Specification for Soft Infant and Toddler Carriers.
- International Hip Dysplasia Institute. Hip Health in Baby Carriers.
- The UK Sling Consortium. The T.I.C.K.S. Rule for Safe Babywearing.
- National Center for Fatality Review and Prevention. Positional Asphyxia in Sitting Devices.
About the Author: Hafiz Nauman Baig is a PhD Scholar in Zoology specializing in Fisheries at Quaid-i-Azam University. Leveraging advanced statistical data analysis in R Studio and research expertise in aquatic adaptation and oxidative stress, he provides rigorous, evidence-based safety and ergonomic evaluations for baby gear.