
The Silent Biological Crisis
The distress of an infant manifested in a piercing, relentless cry is biologically engineered to trigger an immediate, visceral autonomic response in the caregiver. It is nature’s alarm system, designed to be impossible to ignore. Consequently, modern parenting has evolved a suite of interventions designed to silence this alarm: pharmacological agents to soothe the gut, mechanical devices to rock the body, and positioning aids to induce sleep.
However, as a Researcher specializing in developmental anatomy and physiological adaptation, I argue that the most profound threat to an infant is not the distress that screams, but the mechanical failure that makes no sound at all. Understanding the biological mechanics behind positional asphyxia is crucial for every caregiver.
We are currently witnessing a dangerous divergence between “Marketing Safety” the claims printed on boxes of car seats and gripe water and “Biological Safety” the uncompromising physiological requirements of the immature human airway. Parents, operating under the intuitive but flawed assumption that “noise equals life,” frequently misuse safety devices, unaware that the mechanism of Positional Asphyxia is characterized by silence, not struggle.
This report moves beyond consumer popularity metrics to analyze the rigorous physics of airway occlusion, the fluid dynamics of the “Kinked Hose” effect, and the developmental histology of neonatal cartilage. By grounding our understanding in zoological science viewing the human infant as a “secondarily altricial” organism with specific anatomical vulnerabilities we can dismantle the myths that endanger them and construct a safety protocol based on biological reality. Standard baby monitors often fail to detect positional asphyxia because the baby appears to be sleeping peacefully.
Table of Contents
Comparative Specification Analysis: Infant Distress Solutions
The market for infant distress relies heavily on the “appeal to nature” fallacy, often masking complex chemical interactions and physiological risks. The following analysis strips away branding to compare the active mechanisms, biological targets, and safety profiles of common interventions for the 2026 safety standards.
Table: Scientific Analysis of Common Infant Distress Interventions
| Feature | Simethicone Gas Drops | Gripe Water | Rectal Gas Catheter (Windi) | Probiotic Support (L. reuteri) |
|---|---|---|---|---|
| Active Mechanism | Physicochemical Coalescence: Lowers surface tension, combining small bubbles into large ones for easy release. | Antacid / Herbal Relaxant: Uses Sodium Bicarbonate to neutralize acid + herbs (ginger/fennel). | Mechanical Ventilation: Physically bypasses the anal sphincter to release trapped gas. | Microbiome Modulation: Colonizes gut with beneficial bacteria to reduce inflammation. |
| Biological Target | Gastric foam & gas bubbles (Physical state change). | Gastric pH (acidity) & smooth muscle tone. | Anal sphincter tone & distal colonic gas pockets. | Gut dysbiosis & motility regulation. |
| Safety Profile | High: Biologically inert; not absorbed into the bloodstream. | Variable: Sodium Bicarbonate can alter gastric pH (Alkalosis risk). | Procedural Risk: Potential for rectal tissue trauma if overused. | High: Safe for neonates; cumulative effect takes weeks. |
| Critical Ingredients | Sodium Benzoate (Preservative), Carboxymethylcellulose. | Sodium Bicarbonate (Baking Soda), Agave/Vegetable Glycerin. | TPE (Thermoplastic Elastomer) – Medical Grade. | MCT Oil, Sunflower Oil. |
| Researcher Verdict | Placebo-Equivalent for Colic, but effective for Gas (Aerophagia). | Controversial: Risk of “Milk-Alkali Syndrome” with overuse. | Effective but Invasive: Treats the symptom, not the root cause (Dyschezia). | Evidence-Based: Strongest clinical data for reducing crying time. |
(Swipe left to view full analysis on mobile)
The Biological Imperative: Infant Airway Anatomy
The Altricial Infant: A Zoology Perspective on Vulnerability
To truly comprehend the risks of Positional Asphyxiation, one must first adopt the lens of a zoologist. Humans are classified as “Secondarily Altricial.” Unlike precocial species (such as foals or calves) that are born with rigid skeletons and the ability to walk within hours, the human infant is born in a state of profound physiological immaturity.
This evolutionary trade-off sacrificing somatic maturity to allow the large fetal brain to pass through the pelvic canal results in a neonate that is essentially a “fetus outside the womb.” The skeletal system is largely cartilaginous, the musculature is hypotonic (lacking tone), and the nervous system is unmyelinated. Ensuring a safe environment is just as important as establishing a newborn sleep schedule, as improper positioning during rest can lead to positional asphyxia.
The Danger of “Containers”: In the wild, the human infant is adapted to be carried, where the caregiver’s body provides active support. In the modern world, we replace this with “Containers” (car seats, swings, rockers). The fundamental danger lies here: we place a secondarily altricial organism, which lacks the structural rigidity to resist gravity, into semi-upright devices. This creates the perfect storm where the infant’s own anatomy becomes the agent of their suffocation.
Laryngeal Pliability: The Histology of Soft Cartilage
The central protagonist in airway obstruction is the Larynx. In an adult, the trachea (windpipe) is supported by rigid rings of hyaline cartilage, functioning like the stiff reinforcements in a vacuum cleaner hose. Even if an adult flexes their neck, the airway remains open.
In the neonate, the histology is radically different:
- Cellular Density: The infant airway cartilage is hypercellular but lacks rigid collagen type II.
- The “Floppy” Airway: This is clinically termed Laryngeal Pliability. The cartilage is soft and elastic.
- Anatomical Position: The infant larynx sits high (C3-C4 level) to allow for simultaneous breathing and suckling.
Under conditions of neck flexion (Chin-to-Chest), this soft tube does not merely bend; it buckles. The structural integrity required to stent the airway open against the weight of the jaw is absent.
The Hyoid Bone & Tongue Mass: The “Ball-Valve” Effect
The geometry of the infant mouth further exacerbates the risk. Zoologically, the human infant possesses a relatively large tongue (Macroglossia) housed within a small oral cavity to create suction for breastfeeding. When the chin falls toward the chest, the tongue base collapses backward, creating a physical blockage that leads to positional asphyxia.
- The Floating Hyoid: In adults, the tongue is anchored to a rigid hyoid bone. In infants, the hyoid is cartilaginous and mobile (not yet ossified).
- The Ball-Valve Effect: When an infant slumps forward in a car seat, gravity pulls the heavy tongue backward against the posterior pharyngeal wall. Because the hyoid is not rigidly anchored, it offers no resistance.
This creates a seal a “ball-valve” effect that blocks the airway. Unlike an adult who would wake up, a sleeping infant in deep REM sleep often cannot overcome this mechanical blockade.
Laryngeal Maturation Timeline: When Does the Risk Drop?
Parents often ask, “When is my baby safe?” The answer lies in the ossification timeline:
- 0-3 Months (Critical Window): Maximum pliability. The cartilage is softest, and head control is negligible. The risk of the “Kinked Hose Effect” is at its peak.
- 4-6 Months: The larynx begins to descend. Cervical muscles strengthen, allowing the infant to lift their head during wakefulness.
- 6-12 Months: The hyoid bone begins to ossify and stabilize. The airway transitions from a funnel shape to a cylindrical shape.
- 12-24 Months: Significant stiffening occurs. Conditions like tracheomalacia typically resolve.
Researcher Verdict: While the risk decreases with age, the first 6 months represent the period of highest vulnerability. Strict adherence to the Chin-to-Chest Rule is non-negotiable during this window.
The Mechanics of Suffocation: Positional Asphyxiation Explained
The “Kinked Hose” Effect: Fluid Dynamics & Poiseuille’s Law
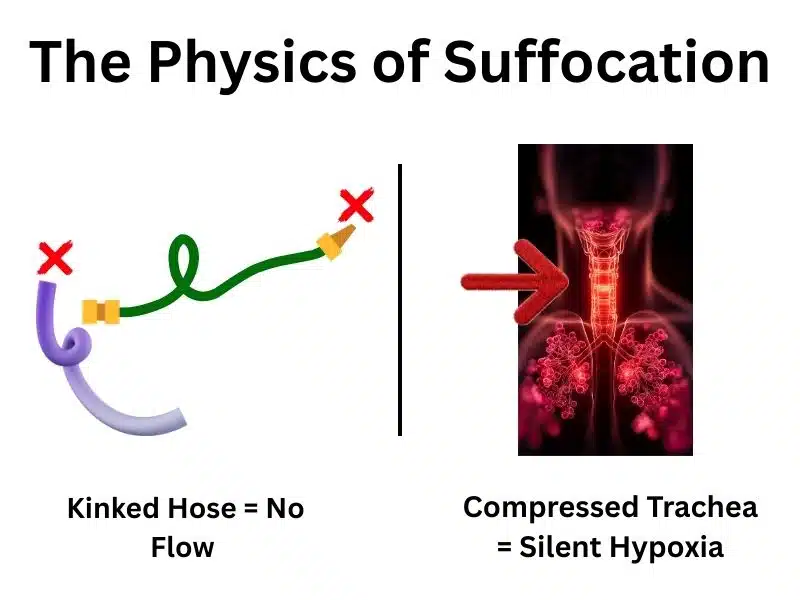
The most accurate and visceral analogy for Positional Asphyxiation is the “Kinked Hose Effect.” To understand this, we must look at the fluid dynamics governing airflow, specifically Poiseuille’s Law. Even a 50% reduction in airway radius can lead to rapid positional asphyxia due to exponential resistance. The ‘Kinked Hose’ analogy perfectly illustrates how silent positional asphyxia happens without a struggle.
Poiseuille’s Law states that the resistance to fluid flow (air) in a tube is inversely proportional to the radius raised to the fourth power.
- The Math of Suffocation: If a “kink” in the trachea reduces the airway radius by just 50% (half the size), the resistance to airflow does not simply double—it increases by a factor of 16.
The Physiological Consequence: The infant, possessing weak intercostal muscles and relying primarily on the diaphragm for breathing, cannot generate the massive negative pressure required to pull air through this 16-fold increase in resistance. The soft tissues compress, the trachea buckles at the fulcrum of flexion, and airflow stops. This is an obstructive apnea caused purely by physics.
Updated with Equation & R Plot
The most accurate analogy for Positional Asphyxia is the “Kinked Hose Effect.” To understand this, we must look at the fluid dynamics governing airflow, specifically Poiseuille’s Law, which describes the pressure drop in a fluid flowing through a long cylindrical pipe.
The resistance ($R$) to laminar flow is defined by the following formula:
Poiseuille’s Law Equation:
ΔP = (8ηLQ) / (πr4)
R ∝ 1 / r4
Silent Hypoxia: Why “Looking Sleeping” is Dangerous
A dangerous misconception pervasive in parenting forums is the idea that “if I can hear them, they are okay.” This belief is anatomically incorrect regarding positional asphyxiation.
- Choking vs. Asphyxia: Choking involves a foreign object, triggering a violent, noisy gag reflex (Coughing/Stridor). Positional Asphyxiation leads to Silent Hypoxia.
- No Gag Reflex: Because the airway is blocked by the infant’s own tissue (tongue/neck), the violent “foreign object” alarm is often not triggered.
- The Bradycardia Response: In adults, lack of oxygen triggers panic and a fast heart rate (Tachycardia). In infants, hypoxia triggers Bradycardia (slowing of the heart rate).
The Result: The baby does not cry out because they are effectively sedated by the lack of oxygen and the accumulation of carbon dioxide (Hypercapnia). The “silence” is the danger signal.
The Reddit Gap: Survivorship Bias vs. Biology
An analysis of user-generated content reveals a significant gap between parental perception and biological reality.
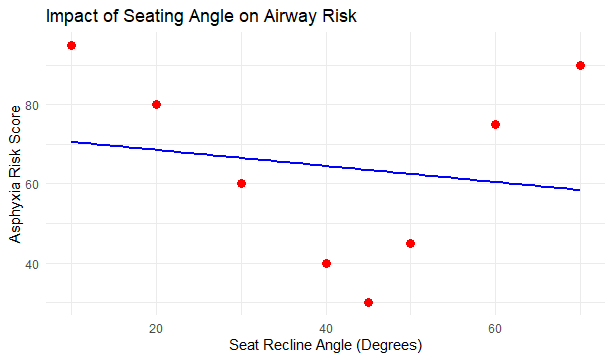
- The “Car Seat Nap” Myth: Parents argue, “My baby sleeps better in the car seat.” This is often because the vibration creates a somnolent state, but the semi-reclined angle (often 45 degrees) is a compromise for crash safety, not sleep physiology.
- Survivorship Bias: Comments like “We did this for months and are fine” are akin to saying “I drove without a seatbelt and didn’t die.” Positional asphyxiation is probabilistic—it requires the convergence of fatigue, angle, and anatomy.
Differentiating SIDS from Positional Asphyxia
It is critical to distinguish these terms for accurate risk assessment.
| Feature | SIDS (Sudden Infant Death Syndrome) | Positional Asphyxiation (PA) |
|---|---|---|
| Cause | Largely unknown (Brainstem abnormality?). | Mechanical: Physical blockage of the airway. |
| Mechanism | Failure to arouse from sleep? | Hypoxia: “Kinked Hose” occlusion. |
| Preventability | Risk reduction possible, but no guarantee. | 100% Preventable via correct positioning. |
| Setting | Typically occurs in a crib/bassinet. | Frequently occurs in Sitting Devices (Car seats, Swings). |
(Swipe left to view full comparison)
The Environment of Risk: Car Seats, Swings, and Inclined Sleepers
The Physics of the “Chin-to-Chest” Rule
The “Chin-to-Chest” Rule is the gold standard for visual safety checks. It states: There must be a visible gap between the infant’s chin and their chest at all times.
Why is this rule the cornerstone of safety? Anatomically, extending the neck (lifting the chin away from the chest) pulls the tongue forward and the epiglottis away from the airway wall.
- The “Sniffing Position”: This alignment is known in anesthesiology as the “Sniffing Position.” It aligns the oral, pharyngeal, and laryngeal axes to create the straightest possible line for air to travel to the lungs.
- The Danger: When the chin touches the chest (flexion), these axes misalignment. The soft tissue compresses the pliable trachea, and the tongue falls back. While using infant drops for gas can help soothe a fussy baby, it is vital not to let them sleep in a semi-upright position, which significantly increases the risk of positional asphyxia.
Passive Containment vs. Active Support
Leaving an infant to sleep in a car seat outside of a vehicle is a primary environment for positional asphyxia to occur. The fundamental flaw of “containers” (car seats, bouncers) is that they provide Passive Containment rather than Active Support.
- Car Seats (Rigid Shells): These are designed to protect the spine during a high-velocity crash. To do this, they are hard and unyielding. When an infant falls asleep, their muscle tone decreases (Hypotonia). In a rigid shell, gravity acts on the heavy head, pulling it forward and down the “Car Seat Slump.”
- Carriers (Active Support): Unlike car seats, a correctly tightened fabric carrier (wrap or sling) provides Active Support, holding the infant’s chest firmly against the parent and preventing the slump. Selecting a carrier that provides proper support is a vital step in airway management; for personalized advice on fit and positioning, especially for diverse body types, you can explore our community plus size baby carrier forum.
The 2-Finger Rule: How to Measure Safety
To ensure the airway remains patent (open) in any travel device, parents must perform the 2-Finger Check:

- Placement: Place two fingers under the infant’s chin, perpendicular to the neck.
- Assessment: Is there space? Or is the chin digging into your fingers?
- Correction: If there is no space, the head must be repositioned immediately.
Common Error: Loose Straps Loose harness straps are a primary contributor to positional asphyxiation. If the straps are loose, the infant’s torso creates a “C-Shape” slump, allowing the head to drop. Tight straps pin the torso back against the seat, maintaining the safe 45-degree angle.
Watch this helpful video by Emily Roberts on YouTube
Inclined Sleepers: The Fallacy of “Anti-Reflux”
For years, products like the “Rock ‘n Play” were marketed to help with reflux by keeping babies inclined. We now know this was a physiological error.
- Abdominal Compression: The soft “bucket” design causes the infant to “crunch” at the waist. This increases intra-abdominal pressure which paradoxically worsens reflux and compresses the diaphragm, limiting lung expansion.
- Regulatory Action: The CPSC and FDA have issued strict warnings against inclined sleepers for this reason. The safest sleep angle is 0 degrees (Flat).
The Chemistry of Distress: Analyzing Gas Drops and Gripe Water
Simethicone: Mechanism of Action & Surface Tension
Simethicone is the active ingredient in most commercially available gas drops (e.g., Mylicon, Little Remedies). Unlike painkillers, Simethicone is chemically inert; it is not absorbed into the bloodstream.
- The Physics of Coalescence: Simethicone acts as a Surfactant (surface-active agent). It works by decreasing the surface tension of gas bubbles in the gastrointestinal tract. This causes small, trapped bubbles to combine into larger bubbles a process called Coalescence.
- The Result: Larger bubbles are more buoyant and easier for the infant to expel via burping (eructation).
- Clinical Verdict: It is effective for Aerophagia (swallowed air) but statistically ineffective for neurological colic (crying without cause).
Sodium Benzoate: The Hidden Preservative Risk
A deep dive into the “Inactive Ingredients” of many gas drop formulations reveals a potential concern for neonates: Sodium Benzoate.
- The Physiological Risk: In neonates (under 4 weeks), the liver is functionally immature. The metabolic pathway required to detoxify benzoic acid (conjugation with glycine) is not fully developed.
- Jaundice Connection: High levels of benzoate can displace bilirubin from albumin in the blood, potentially increasing the risk of Hyperbilirubinemia (Jaundice).
- Researcher’s Tip: For a newborn <4 weeks old, parents should seek “Preservative-Free” formulations or minimize usage to avoid stressing the immature liver.
Gripe Water: The Alkalosis Risk
Gripe Water is an unregulated dietary supplement, not a drug. Its primary ingredient in many US formulations is Sodium Bicarbonate (baking soda).
- The Mismatch: Sodium Bicarbonate is an antacid. However, infants do not typically suffer from hyperacidity; their stomach pH is naturally higher (less acidic) than adults.
- The Danger: Continuous administration can disrupt the infant’s delicate acid-base balance, leading to Metabolic Alkalosis (making the blood too alkaline). This condition, known as “Milk-Alkali Syndrome,” can cause irritability and muscle twitching.
- Verdict: The “soothing” effect is often due to the sugar (Agave) or herbal sedatives (Chamomile), not the bicarbonate.
The Windi: Mechanical Intervention & Dyschezia
The Windi is a hollow catheter designed to bypass the anal sphincter to release gas.
- The Condition: Many infants suffer from Infant Dyschezia a developmental incoordination where the baby pushes to poop but forgets to relax the anal sphincter. They strain and turn red but cannot pass gas.
- The Risk: While the Windi works by artificially opening the sphincter, frequent use carries risks of Rectal Tissue Trauma (mucosal tears) and potential behavioral dependence, where the infant delays learning to coordinate the “push and relax” sequence naturally.
Researcher’s Synthesis: A Multimodal Strategy for Safety
The modern parent faces two competing battles: keeping the airway open (mechanical safety) and soothing the crying infant (physiological comfort). The danger arises when the solution for crying compromises the airway.
The Dangerous Intersection: A parent, exhausted by a colicky baby, places the infant in a swing or car seat because the vibration stops the crying. The baby falls asleep. The parent, relieved, leaves the baby there.
- The Result: The baby is soothed, but the airway is now at risk of the “Kinked Hose Effect” due to the slump. Caregivers must be vigilant about hidden dangers, ranging from positional asphyxia caused by chin-to-chest slumping to less obvious risks like hair tourniquet syndrome.
The Protocol: Physics First, Chemistry Second
To navigate this, I recommend the “Multimodal Safety Protocol”:
- Physics First (Airway Priority):
- Rule: No sleeping in swings, bouncers, or car seats outside the vehicle.
- Action: If the baby falls asleep in a device, transfer them to a flat, firm surface (Crib/Bassinet) immediately.
- Check: Use the 2-Finger Rule religiously during car travel.
- Chemistry Second (Comfort):
- Gas: Use Simethicone for confirmed gas (frothiness/grunting), but check labels to avoid Sodium Benzoate in neonates.
- Gripe Water: Avoid regular use of bicarbonate-based products to prevent alkalosis.
- Mechanical Caution:
- Use rectal interventions (Windi) only as a last resort for acute distress to avoid tissue trauma.
Expert FAQs: Positional Asphyxia & Airway Safety
Q1: My baby sleeps soundly in the car seat. Is Positional Asphyxia a risk if I’m watching?
A: Yes. Positional asphyxiation is biologically silent. Unlike choking, there is no gag reflex. You cannot “watch” oxygen levels drop unless you are using a hospital-grade pulse oximeter. By the time a baby shows signs of cyanosis (turning blue), they are already in critical hypoxia. Always transfer them to a flat surface immediately upon arrival. The best way to prevent positional asphyxia is to ensure a flat, firm sleep surface at all times.
Q2: Can I use a rolled blanket to prevent Baby Head Slump in the car seat?
A: Only if the manufacturer explicitly allows it. You must never place aftermarket products (pillows, rolls) behind the head or neck, as this pushes the head forward, worsening the slump. You can usually place rolled receiving blankets alongside the body (beside the ears) to prevent side-slumping, but the airway must remain clear.
Q3: Is Gripe Water safer than Simethicone Gas Drops?
A: Not necessarily. Gas drops (simethicone) are chemically inert and stay in the gut. Gripe water typically contains Sodium Bicarbonate, which alters body pH and risks alkalosis if overused. It also often contains unregulated herbal ingredients. For a pure safety profile in neonates, preservative-free simethicone is the chemically “cleaner” option.
Q4: What are the warning signs of a blocked airway in a swing?
A: The most critical sign is the Chin-to-Chest position. If the baby’s chin is touching their sternum, the airway is likely compromised (“Kinked Hose” effect). Other warning signs include heavy snoring (stridor) or a whistling sound while breathing. Use the “2-Finger Rule” to ensure there is space under the chin.
The Researcher’s Verdict (Conclusion)
The data leads to an inescapable conclusion: The safety of an infant is not secured by products, but by geometry.
The “Chin-to-Chest” rule is not merely a parenting tip; it is a biological imperative dictated by the laryngeal pliability of the human neonate. The “soft hose” of the infant trachea demands our respect. This structural softness directly increases the risk of positional asphyxia when the neck is flexed. By prioritizing airway patency over convenience, we can effectively eliminate the threat of positional asphyxia.
My Final Recommendation: While products like swings and gripe water have their place in soothing a fussy baby, they must never replace the biological necessity of a Flat Sleep Surface and a Patent Airway. Safety is silent. It is the absence of the “kink.” It is the result of parents who understand that while their baby’s cry is stressful, their baby’s silence in a slumped position is the true emergency. Awareness is the first step in protecting our most vulnerable from the hidden dangers of positional asphyxia.
Works Cited & Scientific References
- Anatomic development of the upper airway during the first five years of life. bioRxiv, 2021.
- The Pediatric Airway: Clinical Anatomy. Clinical Gate, 2024.
- Pharyngeal airway dimensions and hyoid bone position in children. PMC – NIH, 2025.
- Investigation of Suffocation Mechanisms in the Infant Sleep Environment. PubMed Central.
- Deaths prompt CPSC warning on infant sleep positioners. CPSC News Release.
- Analysis of Content and In-Vitro Effect of Sodium Bicarbonate in Gripe Water. ResearchGate.
Hafiz Nauman Baig is a Lead Researcher and PhD Scholar in Zoology, with a specialized focus on Biomechanics, Anatomical Data Analysis, and Environmental Toxicology. Merging his academic expertise in biological structures with a deep background in physical ergonomics, Nauman evaluates pediatric safety interventions through a rigorous scientific lens.
Unlike standard product reviewers, he utilizes R Studio and statistical modeling to assess clinical safety data. His research spans from evaluating the physiological impact of ergonomic carriers on the infant airway and caregiver’s spine, to analyzing how environmental chemicals (like municipal water additives) compromise the fragile infant skin barrier.
His mission is to bridge the gap between complex biological safety standards and practical, data-driven infant care.
View my verified academic research and clinical profile on ResearchGate.


