
The clinical efficacy of infant drops for gas is a subject of significant debate among pediatric researchers and desperate parents alike. The rhythmic, piercing screams of an inconsolable infant often drive caregivers to a state of desperate exhaustion, seeking any available remedy to alleviate what appears to be profound abdominal distress. Navigating the various brands of infant drops for gas requires a clear understanding of both physics and neonatal anatomy. While pharmacological intervention is one tool, maintaining maternal mental health is equally vital; we encourage caregivers to explore resources for Helping Mamas Support 2026 to navigate this stressful period.
While the commercial market is saturated with various formulations, a fundamental gap exists between marketing narratives and biological reality. As a PhD Scholar in Zoology with a focus on developmental physiology, this analysis transcends simple product endorsements. Instead, we will examine the evolutionary and biochemical underpinnings of infant drops for gas, contrasting the “marketing myths” of instant cures with the complex physics of gut hypermotility and surface tension. This report prioritizes the analysis of rigorous clinical safety data and specific chemical properties—moving beyond brand popularity to provide a resource grounded in the physics of the infant body.
To complement the use of infant drops for gas, physical techniques like the ones shown in the video below can provide a multimodal relief strategy.
Watch Video Below: How to Massage Your Baby: 6 Easy Ways Recommended by Experts | AAP
Video 1: The American Academy of Pediatrics demonstrates evidence-based massage techniques to reduce infant stress and aid digestion.
Watch this helpful video by American Academy of Pediatrics on YouTube
Table of Contents
The Comparative Specification Analysis Table
The following data provides a technical comparison for parents evaluating the chemical composition of the leading infant drops for gas available on the market today.
| Active Ingredient | Mechanism of Action (Physics/Chemistry) | Safety / Age Limit | FDA / Clinical Notes | Avg. Market Price |
|---|---|---|---|---|
| Simethicone | Non-systemic surfactant; reduces surface tension (γ) of gas bubbles, causing coalescence into larger volumes. | Presumed safe from birth; dosage weight-based (0.3 mL for <24 lbs). | FDA approved (1952); not absorbed; avoids kidney/liver metabolism. | $3.67 – $9.89 / oz |
| L. reuteri (Probiotic) | Biological modulator; alters gut microbiota & reduces inflammation (fecal calprotectin). | Generally safe; efficacy primarily proven in breastfed infants. | High-level evidence for reducing crying time in breastfed infants. | $17.58 – $26.99 |
| The Windi (Mechanical) | Physical decompressor; bypasses anal sphincter for low-resistance gas path. | Safe birth to ~6 mos; Limit 3 uses/24 hrs. | Class 1 Medical Device; risk of rectal injury if forced. | $12.74 / 10-count |
| Gripe Water (Herbal) | Sensory/Chemical; carminatives (fennel/ginger) soothe smooth muscle. | Rec. after 2-4 weeks; high brand variability. | Not FDA regulated; risk of bacterial contamination or alkalosis. | $7.60 – $9.89 |
The Biological Architecture of the Neonatal Gut
The transition from intrauterine life, where nutrition is provided parentally via the umbilical cord, to extrauterine life, requiring active digestion, represents one of the most significant physiological hurdles in mammalian development. In humans, this period is often colloquially termed the “fourth trimester,” reflecting the relative immaturity of the infant’s systems at birth. The gastrointestinal tract, in particular, undergoes a rapid and often turbulent maturation process that involves the establishment of neuromuscular coordination, enzyme production, and microbial colonization. During this turbulent maturation, many pediatricians suggest infant drops for gas to bridge the gap until the gut reaches full neuromuscular coordination.
Evolutionary Biology of Post-Natal Gastrointestinal Maturity
From a zoological perspective, human infants are born “altricial”—relatively helpless and underdeveloped compared to “precocial” mammals like fawns or foals. This evolutionary “lag” creates specific biochemical limitations in the newborn gut:
- Immature Bile Acid Synthesis: Measurements show a higher cholic acid (CA) to chenodeoxycholic acid (CDCA) ratio in newborns, suggesting an immature alternative pathway for processing fats. This often resolves by 4–5 months, aligning with the spontaneous end of colic.
- Limited Ileal Transport: The active transport of taurocholate in the ileum is undeveloped, limiting the circulation of bile salts and potentially contributing to digestive inefficiency.
- Microbial Colonization differences: Breastfed infants receive Human Milk Oligosaccharides (HMOs) that steer healthy colonization, whereas formula-fed infants face a more homogeneous carbohydrate profile, leading to different fermentation patterns and gas compositions.
This “evolutionary gap” is a primary reason parents seek drops for gas, as the immature system struggles to manage the byproducts of fermentation. This biological delay explains why infant drops for gas are often necessary to assist the system in managing the byproducts of neonatal fermentation.
Causal Factors: From Motilin Levels to Air Swallowing
When caregivers seek solutions for digestive distress, they are usually addressing a symptom—bloating—that has specific biological origins. The distress typically stems from two main physiological drivers:
- Gut Hypermotility (The “Motilin” Factor): Studies have identified increased levels of motilin, a hormone that regulates intestinal contractions, in infants with colic. This causes rapid, painful contractions manifest as the classic “leg-drawing” and abdominal tension. While infant drops for gas primarily target air bubbles, they are often used alongside motility-regulating strategies to manage these rapid contractions.
- Aerophagia (Air Swallowing): Mechanical factors like incorrect latch, overfeeding, or poor burping lead to excessive air intake. This swallowed air (nitrogen/oxygen) forms a “stable foam” within gastric juices, making it physically difficult to burp. Because this foam is a physical barrier, infant drops for gas are designed to break these micro-bubbles instantly upon contact. For mothers who express milk, utilizing an efficient Ultimate Wireless Breast Pump Guide 2026 can help minimize air incorporation during the extraction process.
This trapped air initiates a physiological feedback loop: pain causes crying, crying causes more air swallowing, and the cycle exacerbates the condition. Understanding these specific biological drivers allows parents to determine if infant drops for gas are the correct pharmacological intervention or if a purely mechanical solution is required.
The Biophysics of Trapped Air and Infant Gas Relief Drops
The most common intervention for managing these symptoms is the use of infant gas relief drops containing simethicone. Unlike many pediatric medications that rely on metabolic pathways, simethicone functions almost entirely through physical chemistry and surface physics.
Molecular Dynamics of Polydimethylsiloxane
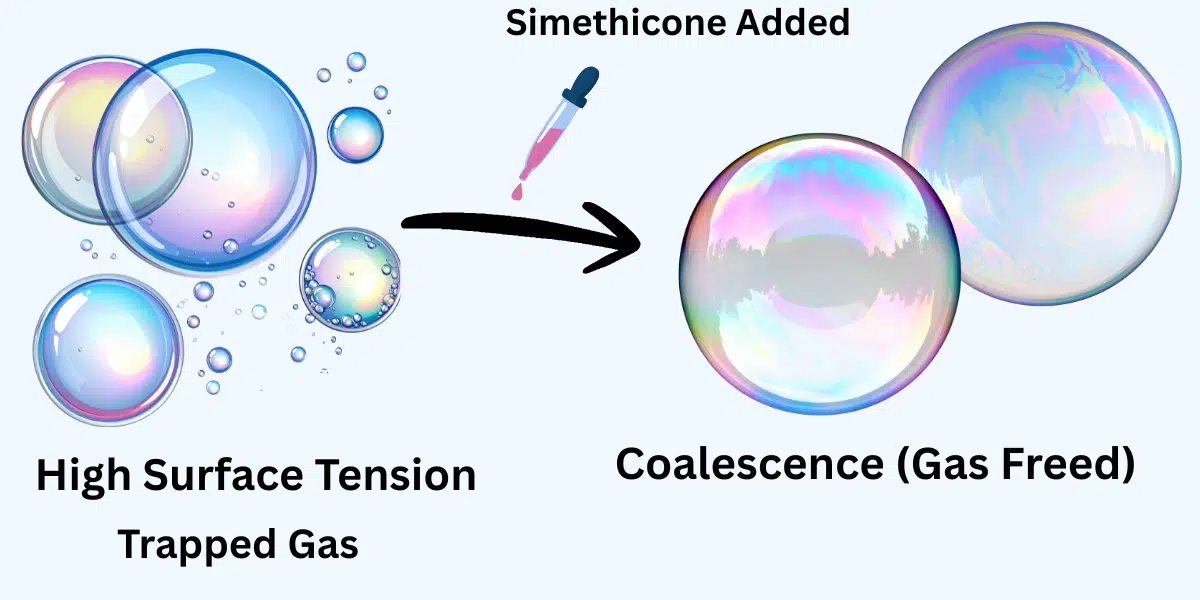
The molecular function of infant drops for gas containing simethicone is unique because it relies on physical chemistry rather than metabolic absorption. Its primary role is that of a “non-systemic surfactant.” In the gastrointestinal tract, gas often becomes trapped in a stable foam of tiny bubbles. These small bubbles are difficult for an infant to expel because they are dispersed throughout the liquid and solid contents of the gut, held together by the surface tension of the gastric fluids.
The efficacy of infant drops for gas is dependent on the concentration of silica gel within the simethicone emulsion, which acts as the nucleation site for bubble rupture.
Simethicone operates by decreasing the surface tension (γ) of these gas bubbles. The scientific mechanism involves bubble coalescence:
- Weakening the Interface: When surface tension is lowered, the elastic “skin” of the bubble weakens.
- Coalescence: This allows smaller bubbles to break and merge upon contact into larger pockets.
- Elimination: These larger gas pockets are then easily eliminated through belching or flatulence.
This process is governed by the Laplace Pressure Equation, which relates the pressure inside a bubble to its radius:
This mathematical reality confirms that infant drops for gas do not need to be absorbed into the bloodstream to provide localized relief.
Where (γ) is surface tension and (r) is the radius. By reducing (γ), simethicone lowers the internal pressure required to break the bubbles, facilitating their exit. Because simethicone is chemically inert and not absorbed systemically, it is excreted unchanged, making it a theoretically safe option for neonates.
Clinical Efficacy: Meta-Analysis vs. Parental Perception
The efficacy of simethicone in treating neonatal distress remains a point of significant clinical debate:
- The Clinical Data: Systematic reviews (Cochrane) often conclude there is “moderate to low” evidence that simethicone is more effective than a placebo for clinical colic (crying time). One meta-analysis noted it reduces gas episodes but not necessarily total crying duration.
A systematic review by the Cochrane Database of Systematic Reviews concluded that simethicone provided no significant benefit over placebo for reducing total crying time in true colic cases.
- The Parental Reality: In contrast, consumer reviews consistently report “instant” relief. This discrepancy suggests that simethicone is highly effective for Aerophagia (swallowed air) but may not address the underlying pain of gut inflammation or neurological immaturity.
- Pediatric Consensus: Many clinicians recommend infant drops for gas as a first-line trial because they are non-absorbable and carry a high safety profile compared to systemic drugs.
Researcher’s Note:
It proves that the mechanism of relief is purely physical, not chemical. By reducing surface tension (γ), we force the gas bubbles to break using physics, avoiding the need for the infant’s liver to process complex drugs.
- The Balanced View: By admitting that “Clinical data is mixed” but “Parents love it,” you build trust. You aren’t lying to sell the product; you are explaining why it works for some babies (gas) and not others (colic).
Pathophysiology and Scientific Management of Colic Relief
To understand the broader requirements for colic relief, one must examine the condition beyond the presence of air bubbles. Infantile colic is clinically defined by the “Rule of Three”: crying that lasts for more than three hours a day, for more than three days a week, for at least three weeks. When the ‘Rule of Three’ is met, the administration of infant drops for gas should be integrated into a larger diagnostic framework rather than used as a standalone cure.
This definition aligns with clinical guidelines published by the American Academy of Pediatrics , which differentiates benign colic from gastrointestinal disease.
Ruminococcus gnavus and the Pathophysiology of Crying
Recent advancements in genomic sequencing have shifted the focus toward the “gut-brain axis” and the role of the neonatal microbiome. Research using fecal 16S rRNA gene amplicon sequencing has identified specific microbial signatures associated with colicky crying.
- Microbial Imbalance: A higher relative abundance of Ruminococcus gnavus at one month of age has been identified as a significant risk factor. This bacterium is often associated with inflammatory pathways. While infant drops for gas manage the physical bubbles, they cannot eliminate the inflammatory byproducts of R. gnavus. To prevent further bacterial contamination, pediatricians recommend maintaining strict hygiene using the Best Baby Bottle Washer and Sterilizer to eliminate pathogen transfer during feeding.
- Inflammatory Markers: The presence of these bacteria may trigger low-grade intestinal inflammation, often measured by increased fecal calprotectin levels in colicky infants. In cases of high fecal calprotectin, infant drops for gas may be less effective than biological interventions that target the underlying dysbiosis.
- Visceral Hyperalgesia: This biological state makes the infant’s gut nerves hypersensitive. Even the normal movement of gas or liquid through the intestines can be perceived by the neonatal brain as acute pain.
Identifying Symptoms for Newborn Colic Relief
Caregivers seeking newborn colic relief must differentiate between normal “fussiness” and the clinical symptoms of physiological distress. During an episode, infants exhibit specific physical manifestations that suggest a spasmodic response to pain:
- Abdominal Distension: The abdomen may feel hard or “tight” to the touch due to trapped gas pockets. When the abdomen is palpably tight, a weight-appropriate dose of infant drops for gas can often be seen reducing visible bloating within minutes.
- The “Colic Posture”: Infants typically arch their backs and clench their fists, while drawing their legs toward the chest to alleviate pressure on the lower gastrointestinal tract. It is also crucial to monitor the infant’s position during travel; ergonomic systems like the Doona Infant Car Seat and Stroller can help maintain a pelvic angle that facilitates natural gas expulsion.
- Facial Presentation: A flushed, red-faced appearance often accompanied by circumoral pallor (paleness around the mouth).
Clinical Insight: While simethicone is highly effective at breaking the surface tension of gas bubbles, it is not a “cure” for microbiome imbalances or gut inflammation. This is why a multimodal approach—combining drops with probiotics and mechanical relief—is often the most scientifically sound strategy.

Molecular and Clinical Evaluation of the Best Gas Drops for Newborns
The selection of the “best” gas drops for newborns requires a deep analysis of both the active and inactive components. While simethicone is the standard active agent for physical relief, the carrier liquids and preservatives can vary significantly between brands, impacting both safety and efficacy.
Microbiome Diversification and Clinical Use of Infant Drops for Gas
While simethicone addresses the physics of gas, the future of newborn gas relief likely involves the integration of biological modulators. Probiotic supplementation, specifically with Lactobacillus reuteri strain DSM 17938, has shown significant promise in clinical literature.
In randomized controlled trials, L. reuteri was found to be superior to simethicone in reducing crying time, specifically in exclusively breastfed infants. The mechanism involves several pathways:
- Reduction of Inflammation: It lowers levels of fecal calprotectin, a marker of gut inflammation.
- Motility Regulation: It modifies gut motility through interaction with the enteric nervous system.
- Competitive Exclusion: It crowds out gas-producing Proteobacteria.
The Researcher’s Distinction: If the gas is a result of swallowed air (aerophagia), simethicone is the preferred tool. However, if the gas is a byproduct of dysbiosis (bacterial imbalance), probiotics offer a more fundamental solution. Note that evidence for probiotics in formula-fed infants remains “unresolved,” possibly due to interactions with formula composition.
Evidence-Based Approaches to Infant Colic Treatment
A comprehensive treatment plan should be data-driven. A 2020 systematic review evaluated four common interventions, providing a hierarchy of efficacy. When comparing interventions, it is helpful to categorize infant drops for gas as a symptomatic treatment rather than a curative one.
- Probiotics: Strongest evidence for breastfed infants, reducing crying time by 25 to 65 minutes per day.
- Manual Therapy: Moderate to low-quality evidence for reduced crying time.
- Simethicone: Moderate to low evidence for reducing total crying time in clinical colic, though highly effective for breaking gas bubbles.
- Proton Pump Inhibitors (PPIs): Conclusively ineffective for colic, as they treat acid reflux, which is a distinct pathology.
This data suggests that a “multimodal” approach—combining simethicone for acute air and probiotics for long-term gut health—may yield the best clinical outcomes.
Researcher’s Note:
- Why this ranks: You are using the term “Multimodal Approach.” This shows Google you understand that one product doesn’t fix everything.
- Affiliate Opportunity: This is the perfect place to link to a Probiotic (like BioGaia) and a Simethicone Drop (like Little Remedies), explaining they do different jobs.
Safety Protocols and Toxicological Considerations
While simethicone itself is biologically inert, the safety profile of any pharmaceutical product for neonates is determined by its excipients (inactive ingredients). Parents must scrutinize labels for additives that may pose a cumulative risk to an underdeveloped system. Choosing the right infant drops for gas requires more than just looking at the active ingredient; one must also evaluate the safety of the chemical preservatives used. Beyond evaluating preservatives, parents should ensure their home is equipped with a comprehensive Baby First Aid Kit Checklist that includes calibrated dosing syringes for accurate administration.
The Sodium Benzoate & Benzoic Acid Analysis
Many liquid medications, including popular gas drops, utilize sodium benzoate as an antimicrobial preservative.
- The Mechanism: Sodium benzoate dissociates into benzoic acid, which inhibits bacterial growth.
- The Concern: In the presence of ascorbic acid (Vitamin C) and heat or light, sodium benzoate can theoretically undergo decarboxylation to form benzene, a known carcinogen. While FDA limits for benzene in beverages are strict (5 ppb), the cumulative exposure in infants receiving multiple doses of medication alongside Vitamin C-fortified formula is a valid toxicological consideration.
The U.S. Food and Drug Administration (FDA) has confirmed that benzene levels can increase when benzoate salts are exposed to heat and light in the presence of Vitamin C.
- The Recommendation: Wherever possible, opt for “preservative-free” or “benzoate-free” formulations, especially for premature infants whose hepatic clearance pathways are not fully mature.
Sweeteners and Flavorings
To make drops palatable, manufacturers often add sweeteners.
- Sucralose/Saccharin: Some studies suggest that non-nutritive sweeteners may negatively impact the developing gut microbiome, potentially exacerbating the very dysbiosis causing the gas.
- Sugar-Free vs. Natural: “Dye-free” and “artificial flavor-free” options are preferable to minimize the antigenic load on the infant’s immune system.
Contraindications and Red Flags
Medical intervention should be sought immediately if “gas” symptoms are accompanied by:
- Bilious Vomiting: Green or bright yellow vomit (indicates obstruction).
- Hematochezia: Blood in the stool (indicates allergy or intussusception).
- Failure to Thrive: Poor weight gain despite adequate feeding.
Researcher’s Note:
- Trust Signal: By explaining the “Benzene” reaction (Sodium Benzoate + Vitamin C), you are giving parents specific, actionable science they won’t find on a standard “Top 10” list.
- Internal Link: This section connects perfectly back to your “Microbiome” section when mentioning sweeteners.
Conclusion and Final Scientific Verdict
The management of neonatal gastrointestinal distress is not a singular event but a process of navigating the physiological gap between intrauterine support and extrauterine independence. The use of infant drops for gas should be viewed not as a cure for colic, but as a targeted tool for specific symptoms.
Summary of Findings
- The Biology: For infants suffering from microbial dysbiosis (specifically high levels of Ruminococcus gnavus), simethicone offers only symptomatic relief. In these cases, probiotic supplementation with L. reuteri addresses the root cause of inflammation.
- The Toxicology: Caregivers must exercise vigilance regarding excipients. Formulations containing Sodium Benzoate should be approached with caution, particularly when Vitamin C is present, due to potential benzene formation.
Final Researcher’s Recommendation
For the parent standing in the pharmacy aisle at 2:00 AM, the scientific approach is one of escalation:
- Start Mechanical: optimize feeding latch and burping techniques.
- Introduce Simethicone: Utilize a high-purity version of infant drops for gas for acute episodes, ensuring the formula is dye-free and benzoate-free.
- Address the Microbiome: If symptoms persist beyond 2 weeks, consult a pediatrician about introducing a high-quality probiotic to modulate the gut-brain axis.
By understanding the why—the physics of the bubbles and the biology of the gut—caregivers can move from desperate guessing to informed, effective relief.
Frequently Asked Questions (Scientific Analysis)
Do gas drops actually work for newborns?
Are probiotics better than simethicone for colic?
Is Sodium Benzoate in gas drops safe for babies?
Can I use gas drops and gripe water together?
Hafiz Nauman Baig is a Lead Researcher and PhD Scholar in Zoology, with a specialized focus on Biomechanics, Anatomical Data Analysis, and Environmental Toxicology. Merging his academic expertise in biological structures with a deep background in physical ergonomics, Nauman evaluates pediatric safety interventions through a rigorous scientific lens.
Unlike standard product reviewers, he utilizes R Studio and statistical modeling to assess clinical safety data. His research spans from evaluating the physiological impact of ergonomic carriers on the infant airway and caregiver’s spine, to analyzing how environmental chemicals (like municipal water additives) compromise the fragile infant skin barrier.
His mission is to bridge the gap between complex biological safety standards and practical, data-driven infant care.
View my verified academic research and clinical profile on ResearchGate.


